10 Back Pain Myths About Aging That Need to Go
Back pain is common in older adults. But common does not mean normal, inevitable, or something that should be met with fear.


Unfortunately, many older adults are still told things like, “Your spine is just worn out,” “You should stop bending and lifting,” or “At your age, you probably need imaging, injections, or surgery.” These messages may sound reasonable, but they often lead people in the wrong direction.
A 2025 review published in Chiropractic & Manual Therapies, challenges ten of the most persistent myths about low back pain in older adults and explains how these misconceptions can drive ineffective, costly, and sometimes harmful care. The bigger message is not that back pain should be ignored. It is that older adults deserve better, more evidence-based care that focuses on function, confidence, and the whole person rather than fear-based assumptions about aging.
Why this matters
Low back pain is one of the most disabling conditions affecting older adults, and it also carries a major cost burden for individuals and health systems. Yet one of the most preventable contributors to that burden is misinformation. When people believe their pain automatically means damage, fragility, or decline, they may avoid activity, lose confidence, become less independent, and end up pursuing tests or treatments that are unlikely to help. The review argues that myths around aging and back pain can shape clinical decision-making, public attitudes, media messaging, and even health policy in ways that reinforce poor outcomes.
Myth 1: Back pain is inevitable as we age
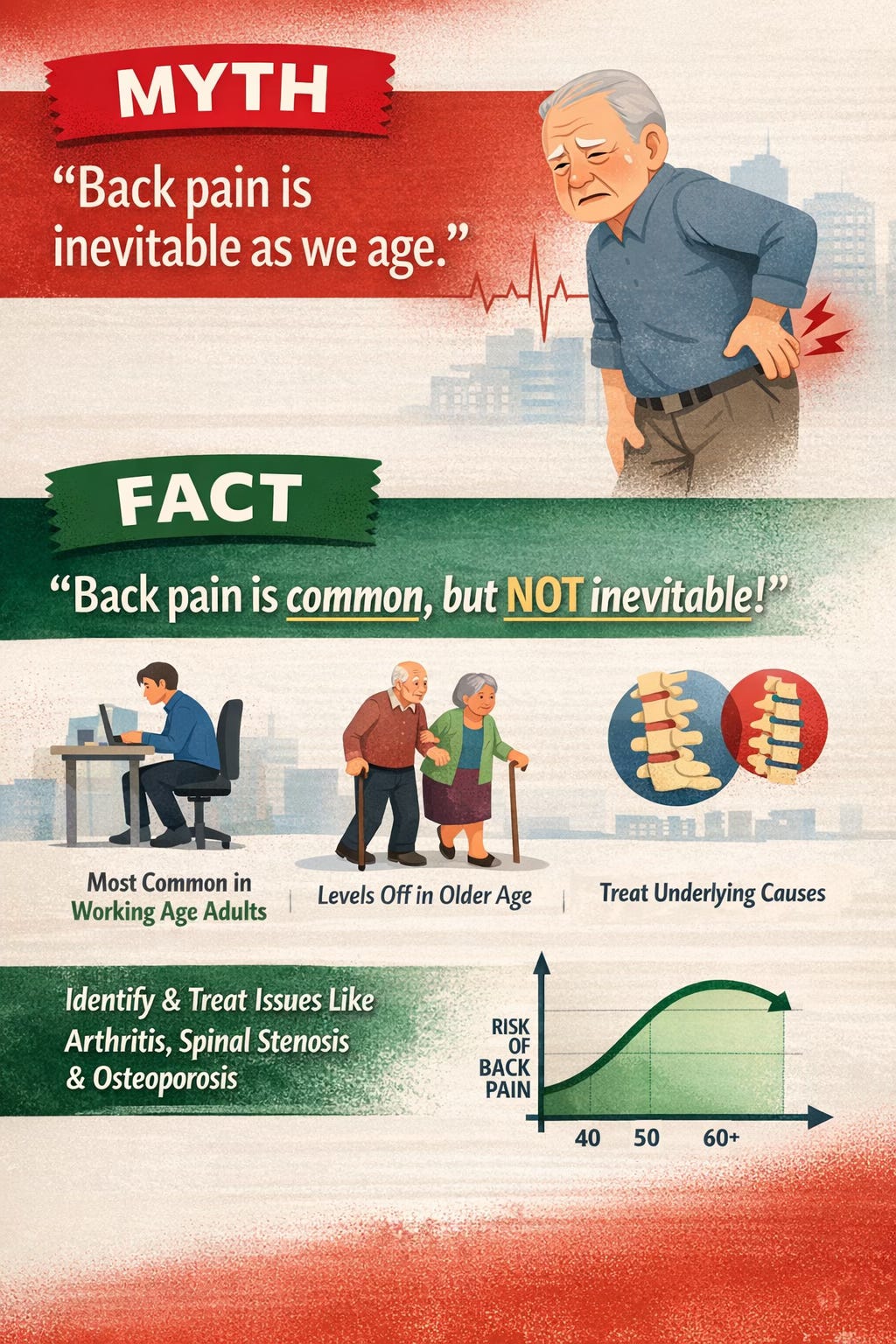
Back pain may be common, but it is not inevitable. The paper notes that non-specific low back pain tends to rise until about age 60, then level off and even slightly decrease. At the same time, some older adults do experience more disability when pain persists, especially when conditions such as osteoarthritis, spinal stenosis, or osteoporosis are involved. That distinction matters. Age alone does not guarantee back pain. It means clinicians should stay alert for specific causes when appropriate, while avoiding the assumption that pain is simply the unavoidable price of getting older.
Myth 2: Back pain in older adults is usually caused by something serious
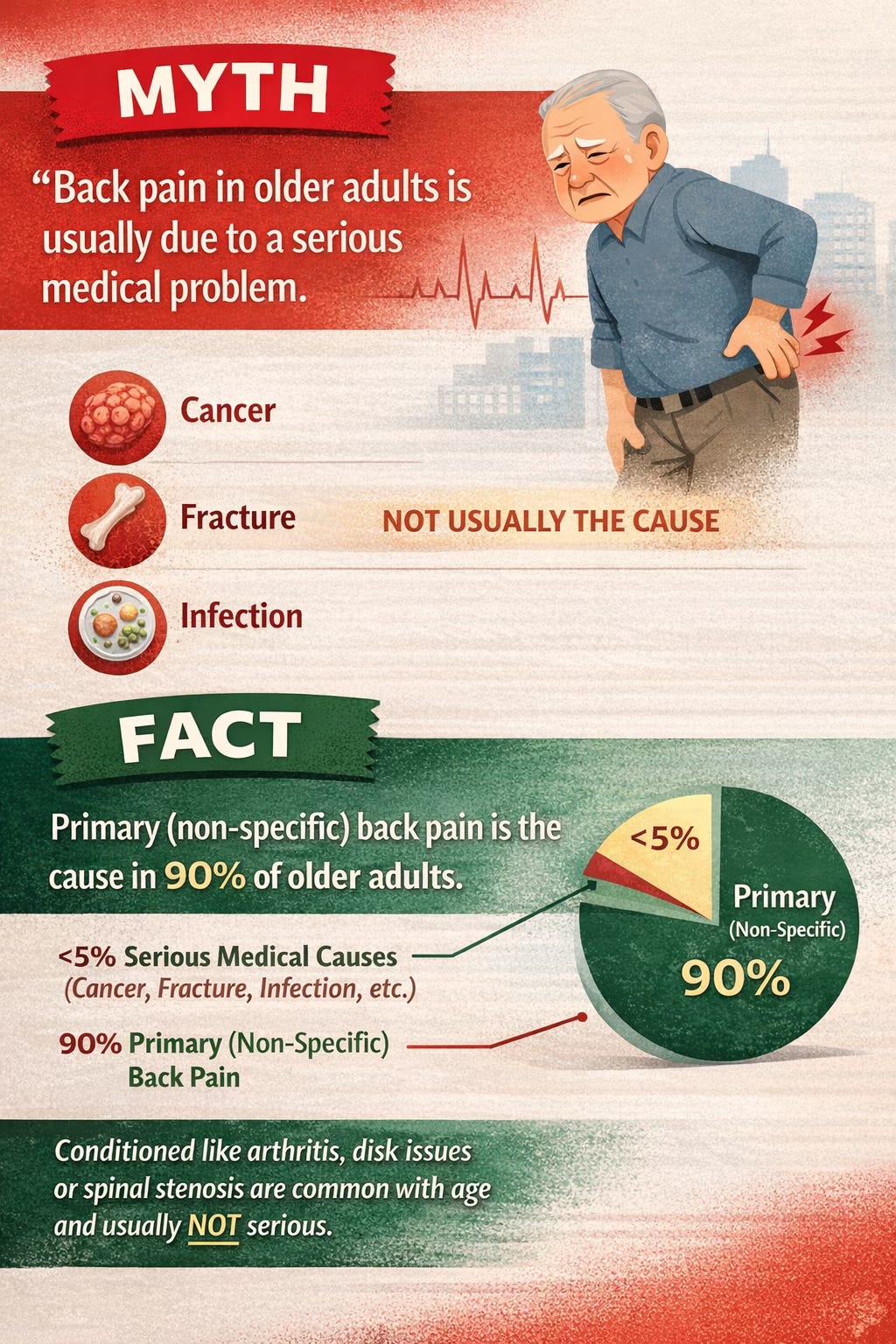
This is one of the most common fears. Many people assume that if an older adult develops back pain, it must be cancer, a fracture, or an infection. Serious causes do exist and must be ruled out when red flags are present, but they account for a small minority of cases. The review notes that primary, or non-specific, low back pain remains the most common type across age groups, including older adults. In other words, most back pain in older adults is still not explained by a dangerous medical condition. That is reassuring, but it also reinforces the importance of thoughtful assessment rather than automatic alarm.
Myth 3: Anyone over 50 with back pain should get imaging
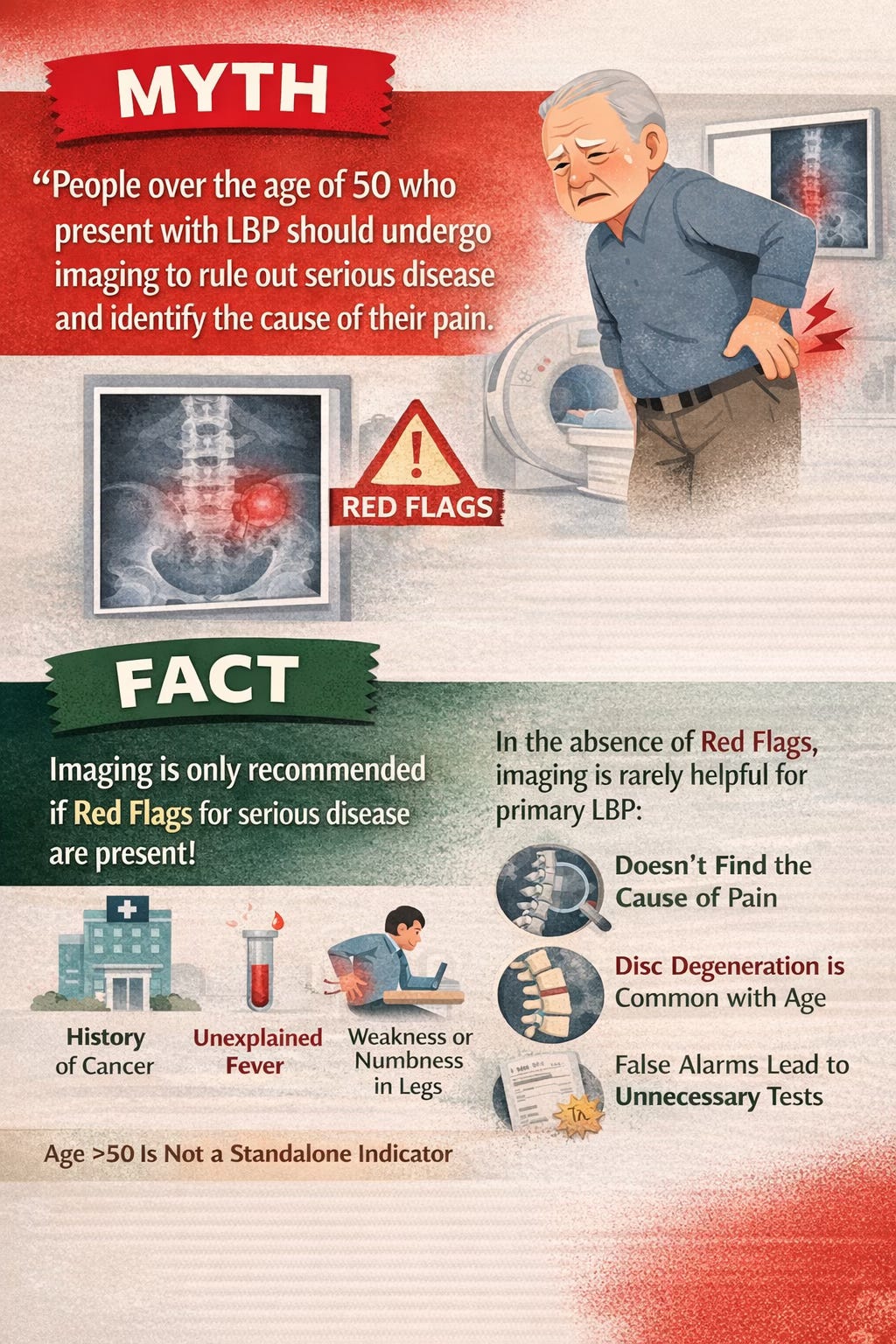
This belief has had remarkable staying power. Yet imaging is not routinely recommended in the absence of red flags. The reason is simple: scans often show age-related changes that may look dramatic but do not actually explain the pain. Degenerative discs, facet joint changes, canal narrowing, and other findings are common even in people who have no symptoms at all. Worse, unnecessary imaging can lead to incidental findings, more specialist referrals, more worry, and more invasive care that does not improve outcomes. Being over 50 should never be treated as a stand-alone reason for imaging. Age is just one piece of the clinical picture.
Myth 4: Older adults with back pain should avoid bending, twisting, and lifting
This message can be deeply harmful. Many people are told to move cautiously, avoid loading the spine, and let pain dictate every decision. But for most people with non-specific back pain, ordinary movement is not causing injury. In fact, avoidance can prolong recovery and increase stiffness, deconditioning, and disability. The paper highlights an important truth: an older spine is not automatically fragile. Bending, twisting, lifting, and gradual loading are normal human movements. With appropriate progression, they help maintain strength, resilience, and confidence. Fear of movement often becomes a bigger problem than movement itself.
Myth 5: Bed rest is recommended
Bed rest is particularly discouraged in older adults. Extended inactivity can contribute to joint stiffness, muscle loss, reduced bone density, pressure injuries, and venous thromboembolism. It can also make people feel older and less capable than they are. Staying as active as possible within reason is generally a better strategy. Walking, light aerobic activity, and strength work can help preserve the physical reserve older adults need to stay independent. The goal is not to push through severe symptoms recklessly, but to avoid the trap of prolonged rest that leaves the body weaker and recovery slower.
Myth 6: Medication should be the first-line treatment
Medication often seems like the simplest starting point, but the evidence is less encouraging than many assume. The review notes that acetaminophen has not shown meaningful benefit over placebo in high-quality trials. NSAIDs may offer only modest benefit and can pose risks in older adults, especially those with hypertension, bleeding risk, or blood thinner use. Muscle relaxants can increase light-headedness. Gabapentinoids such as pregabalin and gabapentin have not performed better than placebo for many forms of back pain and may worsen dizziness and cognitive issues. Some antidepressants offer only limited benefit while carrying their own side effects. In older adults who already take multiple medications, the possibility of harmful interactions becomes even more important. The takeaway is not that medication is never appropriate. It is that it should not be the default foundation of care.
Myth 7: Surgery is effective for back-dominant pain in older adults
This is another area where assumptions often outpace evidence. Surgery is not well supported for primary back-dominant pain when there are no significant radicular leg symptoms. In older adults, the risks are even more relevant because surgical complications rise with age and comorbidity. The paper reports complication rates for spine surgery in older adults ranging from 3% to 29%. At the same time, referrals for surgery continue to rise, often because imaging shows degenerative changes that look impressive but do not necessarily correlate with pain. Surgery may have a role in selected cases involving leg-dominant radicular symptoms, such as certain cases of herniated disc or lumbar spinal stenosis. But even then, improvement in back pain itself is far from guaranteed.
Myth 8: Chronic low back pain is always due to structural damage
This myth can trap people in a lifelong search for “what is broken.” The problem is that most older adults have structural changes on imaging, yet only a small fraction experience chronic disabling back pain. Chronic low back pain is often best understood through a biopsychosocial lens. It may begin with a physical trigger, but ongoing pain can be shaped by fear, low mood, reduced confidence, stress, inactivity, and unhelpful beliefs. In older adults, fear of movement can lead to deconditioning, weight gain, bone loss, and sarcopenia, which then reinforce the pain cycle. Effective care usually requires more than trying to “fix” one structure. It involves addressing habits, beliefs, function, and confidence alongside physical rehabilitation.
Myth 9: Injections and similar procedures are highly effective for chronic back pain
Procedures such as epidural steroid injections, facet injections, nerve blocks, and radiofrequency ablation are widely used, but recent evidence has cast doubt on how much they actually help many patients with chronic spinal pain. The review points to evidence suggesting that these procedures may perform no better than sham procedures for chronic back or radicular pain lasting more than three months. In older adults, risks such as hyperglycemia, bone mineral loss, and temporary weakness may also increase the chance of falls and fractures. These procedures continue to grow in use despite uncertain benefit and substantial cost. That should prompt careful discussion before assuming they are a logical next step.
Myth 10: Disc herniations causing leg pain are very common in older adults
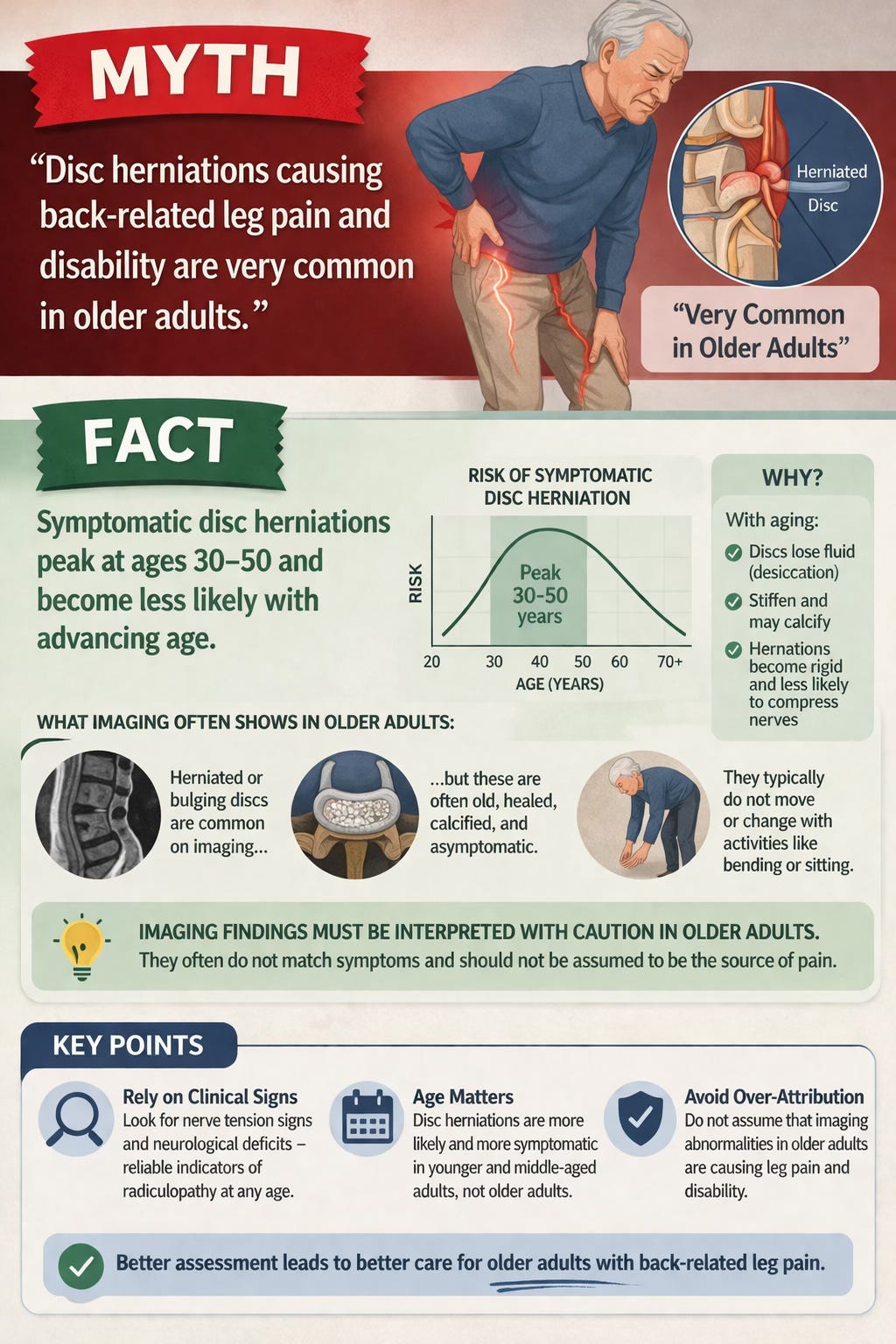
Symptomatic disc herniations actually peak earlier in life, generally between ages 30 and 50. As discs age, they lose water content, stiffen, and may calcify, making them less likely to behave like the classic, mobile herniations often seen in younger adults. Imaging in older adults may still show bulges or herniations, but many of these are old, static, and asymptomatic. That is why scans must be interpreted carefully. In older adults with back-related leg pain, clinical signs such as nerve tension findings and neurological deficits often matter more than the scan alone.
The bigger clinical lesson
When these myths go unchallenged, they can lead to a pattern of care built around fear, overmedicalization, and passivity. That can mean too much imaging, too many procedures, too much focus on structural findings, and not enough attention to movement, confidence, function, and the person’s goals. The review warns that these myths can also fuel ageist assumptions in care, underuse conservative therapies, and fragment interdisciplinary treatment. Social media and popular health messaging can make the problem worse by portraying aging spines as damaged by default.
A better approach is more measured and more hopeful. It starts with careful screening for red flags and specific pathology when appropriate. It continues with evidence-based reassurance, support for staying active, and a management plan that prioritizes function, self-efficacy, and the biopsychosocial realities of pain. It also means recognizing that older adults are not a fragile group who should automatically be steered toward rest, scans, pills, injections, or surgery.
What older adults and families should remember
If you are over 60 and dealing with back pain, it does not automatically mean your spine is failing. It does not automatically mean you need imaging. It does not mean rest is best, and it does not mean surgery or medication should be the first answer. It does mean your pain deserves a proper assessment, especially if there are red flags such as trauma, unexplained weight loss, cancer history, infection signs, major weakness, bowel or bladder changes, or other concerning symptoms. But in many cases, the path forward is more conservative, more active, and more empowering than people expect.
A more useful way to think about back pain and aging
The spine changes with age, just like skin, joints, eyesight, and muscle mass change with age. But age-related change does not automatically equal damage, and damage does not automatically equal pain. The most helpful care often comes from understanding that older adults can still build strength, improve mobility, restore confidence, and function well even when back pain has been present for some time.
That may be the most important message of all: older age is not a reason to become more fearful about back pain. It is a reason to become more precise, more evidence-based, and more thoughtful about how we respond to it.
Reference
Ammendolia, C. (2025). Ten myths of back pain in older adults that can lead to ineffective and harmful care. Chiropractic & Manual Therapies, 33, Article 45. https://doi.org/10.1186/s12998-025-00609-9