
AC Joint Sprain Injuries
What They Are, What the Different Types Mean, and When Treatment Helps


Shoulder injuries can be confusing, especially when you are told you have an “AC joint sprain” or a “shoulder separation.” Many people hear those terms and assume they mean the shoulder has fully dislocated, but that is not usually what is happening. In many cases, the injury involves the acromioclavicular joint, or AC joint, which sits at the top of the shoulder where the collarbone meets part of the shoulder blade called the acromion. This small joint plays an important role in normal shoulder movement, especially when you lift your arm overhead, reach across your body, or absorb force through the shoulder.
An AC joint sprain or separation happens when the ligaments that support this joint are stretched or torn, usually after a direct blow to the outside or top of the shoulder, such as a fall while cycling, skiing, or playing contact sports. It can also happen after a fall onto an outstretched hand or elbow. These injuries are common in athletes and active adults, and some reviews note that AC joint injuries make up a large share of shoulder injuries overall, especially in contact and collision sports.
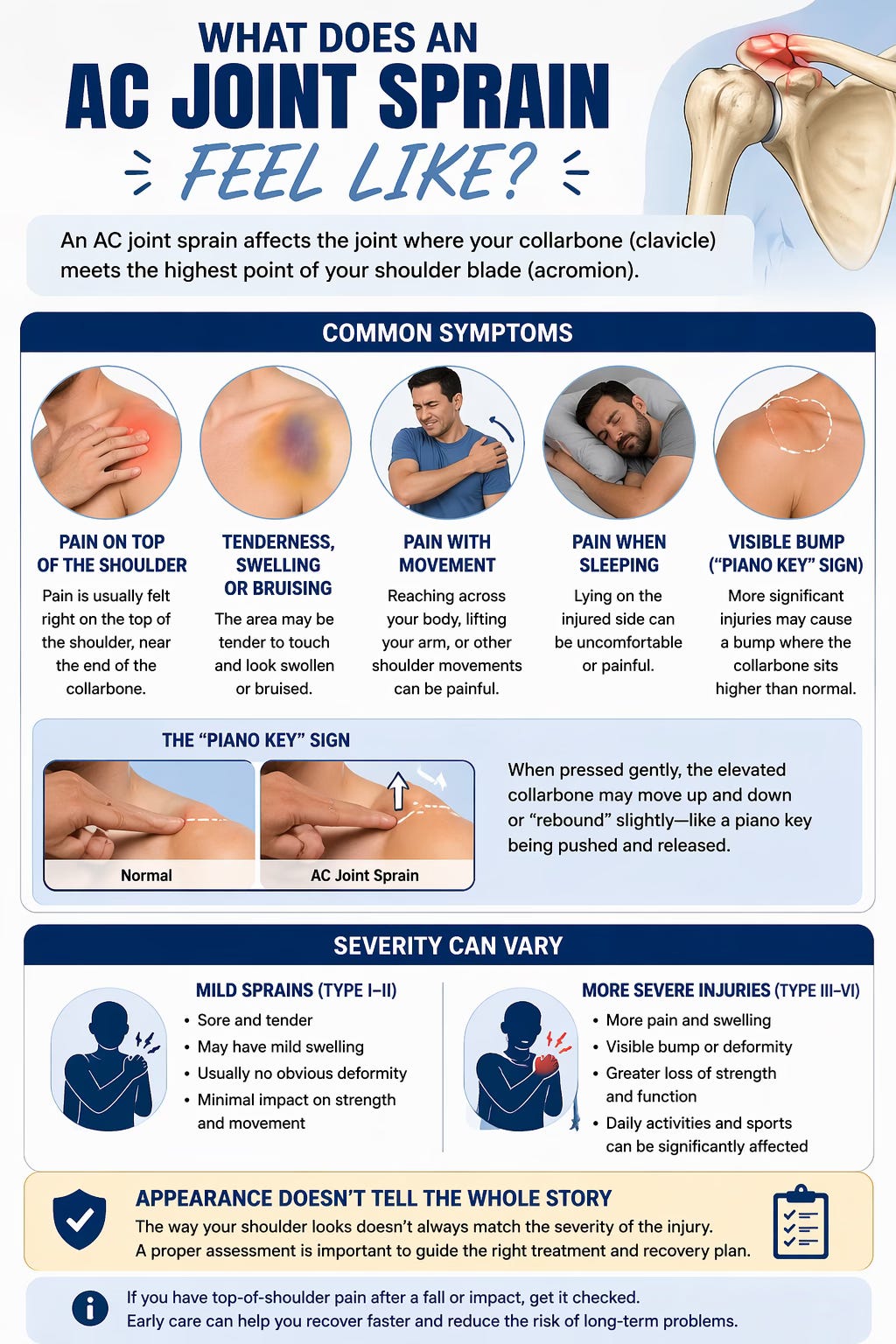
What does an AC joint sprain feel like?
Most people with an AC joint sprain feel pain right on the top of the shoulder, usually near the end of the collarbone. The area may become tender, swollen, or bruised. Shoulder motion can be painful, especially reaching across the body, lifting the arm, or trying to sleep on the injured side. With more significant injuries, there may also be a visible bump at the top of the shoulder where the collarbone sits higher than normal. Clinicians sometimes describe this as a “piano key” sign because the elevated clavicle may move or rebound slightly when pressed.
The severity of symptoms usually depends on how badly the ligaments are injured. Mild sprains can be quite sore but may not look dramatically different. More severe injuries may create obvious deformity and greater loss of shoulder strength or function. Even so, appearance alone does not always tell the whole story, which is why proper assessment matters.
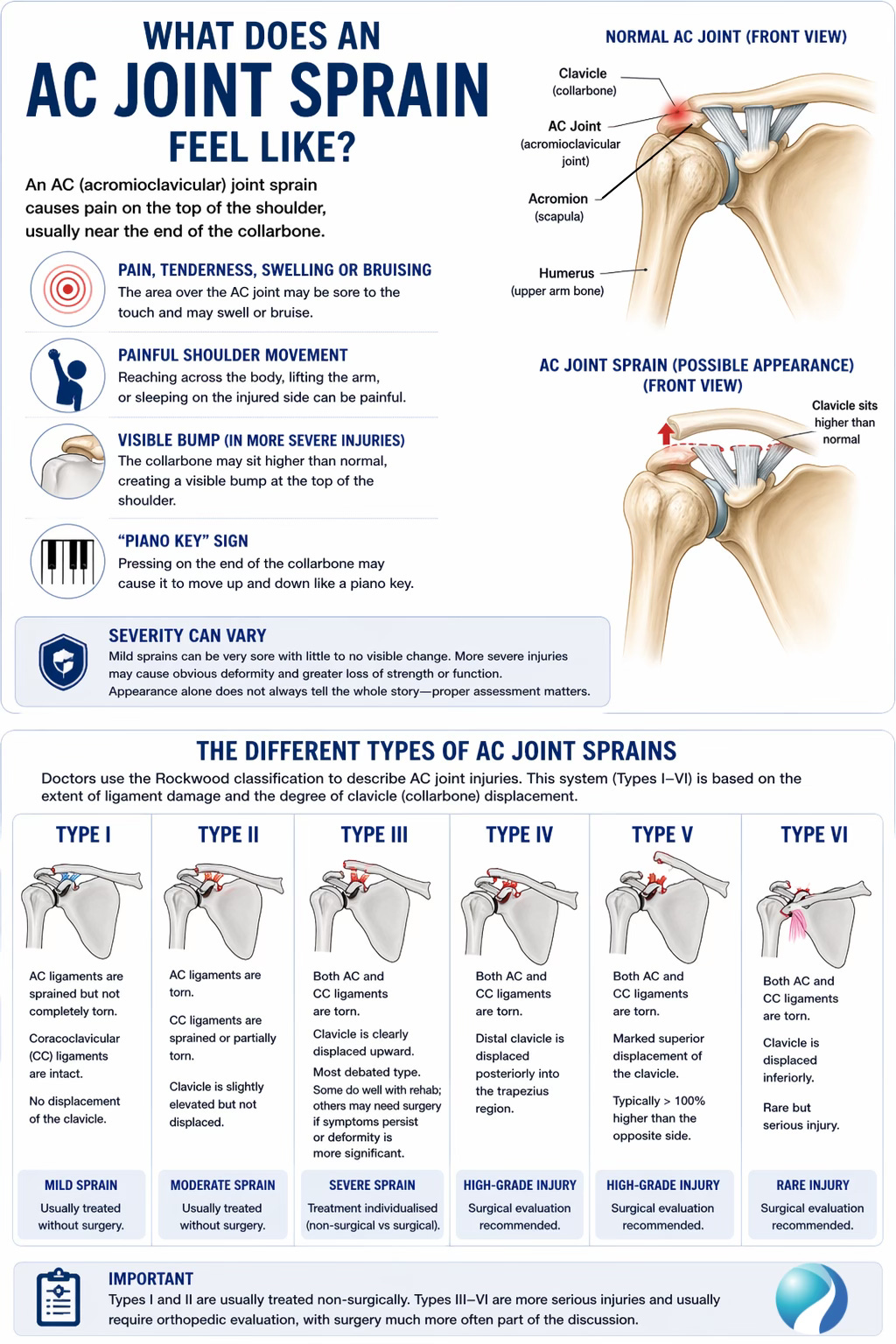
The different types of AC joint sprains
Doctors commonly use the Rockwood classification to describe AC joint injuries. This system divides injuries into types I through VI based on how much ligament damage has occurred and how much the collarbone has shifted. It is considered the standard system used to guide management.
A Type I injury is the mildest form. In this case, the AC ligaments are sprained but not completely torn, the coracoclavicular ligaments are still intact, and there is usually no obvious displacement on x-ray. This is the classic “mild AC sprain.”
A Type II injury means the AC ligaments are torn and the coracoclavicular ligaments are sprained or partially injured, but the clavicle is not dramatically displaced. These are still usually treated without surgery.
A Type III injury is more significant. Here, both the AC and coracoclavicular ligaments are torn, so the collarbone becomes more clearly displaced upward. This is the injury type that causes the most debate because some patients do well with rehabilitation alone, while others, especially certain athletes or workers with high physical demands, may be considered for surgery if symptoms persist or deformity is more substantial.
Types IV, V, and VI are higher-grade injuries. Type IV involves the distal clavicle being pushed backward, often into the trapezius region. Type V involves marked superior displacement, typically greater than 100% compared with the opposite side. Type VI is rare and involves the clavicle being displaced downward into an abnormal position. These higher-grade injuries are generally referred for orthopedic evaluation because surgery is much more often part of the discussion.
How is an AC joint sprain diagnosed?
Diagnosis usually starts with the story of how the injury happened, followed by a physical exam and imaging. Standard shoulder x-rays are often enough to confirm the injury and to rule out other causes of traumatic shoulder pain, such as a fracture. In some cases, special views, comparison films of the other shoulder, or occasionally ultrasound or MRI may be used if the diagnosis is unclear or if the injury appears more complex.
The main goals during assessment are to figure out how severe the injury is, whether there is important displacement, and whether there are any associated injuries that also need attention. That classification matters because it helps determine whether treatment should stay conservative or whether referral for surgical assessment is more appropriate.
Do all AC joint sprains need surgery?
Most AC joint sprains do not need surgery, especially Types I and II, and often Type III as well. Major guidelines and reviews support nonoperative care for lower-grade injuries and recommend that even many Type III injuries begin with a rehabilitation-first approach.
A 2019 Cochrane review found no clear long-term advantage of surgery over conservative treatment for function, return to sport or work, or quality of life at one year, while people treated conservatively often recovered earlier in the short term. The review also found that surgery carried a higher risk of complications, especially complications related to hardware and infection, although some older studies used surgical techniques that are less common today.
That does not mean surgery is never appropriate. Higher-grade injuries, especially Types IV through VI, are usually managed surgically, and some Type III injuries may still be considered for surgery in elite overhead athletes, heavy laborers, or patients with ongoing symptoms or major cosmetic concerns after conservative care. But for many people, especially with Type I, II, and a large number of Type III injuries, nonoperative treatment works very well.
What does conservative treatment involve?
For most AC joint sprains, early treatment focuses on calming pain and protecting the joint. That usually means a sling for comfort, ice, and pain-relieving medication as appropriate. Reviews and practice guidance generally describe a short period of immobilization, often around one to two weeks for milder injuries, followed by a gradual return to motion and progressive rehabilitation.
Once the acute pain settles, rehab becomes very important. Early motion is typically introduced in a controlled way to prevent stiffness, followed by strengthening of the shoulder, rotator cuff, scapular stabilizers, and surrounding musculature. The pace depends on the injury grade, pain level, and the patient’s goals. Lower-grade sprains often recover relatively quickly, while higher-grade injuries can take longer. According to StatPearls, many people regain useful motion by around six weeks and return to normal activity by around 12 weeks after nonoperative care, although timelines can vary.
What about recovery time?
Recovery is not the same for every person, but there are some general patterns. Johns Hopkins notes that a grade 1injury may settle in roughly 10 to 14 days, while a grade 3 injury may take six to eight weeks, with grade 2 somewhere in between. Broader clinical reviews suggest that most people treated nonoperatively recover functional motion within about six weeks and gradually return to regular activities over the following weeks.
The more physically demanding your activities are, the more important it is to make sure motion, strength, and control have returned before going back to full sports or heavy lifting. Returning too quickly can prolong symptoms, especially if the shoulder still feels unstable, weak, or painful across the top.
When should you get assessed?
It is a good idea to get assessed if you have had a fall or shoulder impact and notice pain at the top of the shoulder, swelling, bruising, reduced motion, or a bump near the end of the collarbone. Assessment is especially important if symptoms are not improving, if the deformity is obvious, if you cannot comfortably use the arm, or if the injury happened during a higher-force trauma such as a cycling crash, contact sport collision, or vehicle accident.
It is also worth getting checked because not every painful shoulder after trauma is “just” an AC sprain. Fractures, clavicle injuries, sternoclavicular injuries, rotator cuff injuries, labral injuries, and shoulder dislocations can sometimes overlap or mimic similar symptoms. A proper exam helps make sure the right diagnosis is being treated.
How our clinic can help
At The Muscle & Joint Clinic, we help patients with shoulder injuries by focusing on both the diagnosis and the recovery process. With AC joint sprains, that means helping determine whether the injury appears mild and manageable with conservative care, or whether it may need imaging review or orthopedic referral. Once the diagnosis is clearer, treatment can focus on calming the irritated tissues, restoring comfortable movement, and gradually rebuilding strength and shoulder control.
For patients recovering nonoperatively, care may include activity modification advice, guided mobility work, progressive exercise, soft-tissue and joint-based treatment where appropriate, and return-to-sport or return-to-work planning based on symptoms and function. The goal is not just to wait for pain to settle. The goal is to help the shoulder move well again, tolerate load, and return to day-to-day activity with confidence.
AC joint sprain injuries are common, especially after falls and sports-related impacts, but they vary quite a bit in severity. A mild Type I injury may heal quickly with rest and rehabilitation, while higher-grade injuries require closer monitoring and sometimes surgical consultation. The good news is that most lower-grade AC joint sprains recover well without surgery, and even many Type III injuries can do well with a conservative, rehab-first approach.
If you have pain at the top of the shoulder after a fall, collision, or sports injury, getting it assessed can help you understand what type of AC joint injury you may be dealing with, and what the right next step looks like.
References
Johns Hopkins Medicine. (n.d.). AC joint problems. Johns Hopkins Medicine. Retrieved April 24, 2026, from https://www.hopkinsmedicine.org/health/conditions-and-diseases/ac-joint-problems
Kiel, J., Taqi, M., & Kaiser, K. (2022). Acromioclavicular joint injury. In StatPearls. StatPearls Publishing. Retrieved April 24, 2026, from https://www.ncbi.nlm.nih.gov/books/NBK493188/
Simon, L. M., Nguyen, V., & Ezinwa, N. M. (2023). Acute shoulder injuries in adults. American Family Physician, 107(5), 503–512. https://www.aafp.org/pubs/afp/issues/2023/0500/acute-shoulder-injuries.html
Tamaoki, M. J. S., Lenza, M., Matsunaga, F. T., Belloti, J. C., Matsumoto, M. H., & Faloppa, F. (2019). Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database of Systematic Reviews, 2019(10), CD007429. https://doi.org/10.1002/14651858.CD007429.pub3