
Baker’s Cyst: What It Is And Why It Happens
And How We Can Help!


A Baker’s cyst, also known as a popliteal cyst, is a fluid-filled swelling that develops at the back of the knee. Many patients first notice it as a feeling of tightness, fullness, or pressure behind the knee, especially when bending the knee, standing after sitting, walking for longer periods, or trying to squat or kneel. Some Baker’s cysts are small and painless, while others can become large enough to restrict motion and cause discomfort during everyday activities.
Although the swelling appears behind the knee, a Baker’s cyst is often not the original problem. In many cases, it is a sign that something inside the knee joint is irritated. Conditions such as knee osteoarthritis, meniscal irritation, cartilage wear, joint inflammation, or previous knee injury can cause the knee to produce extra synovial fluid. This extra fluid can move toward the back of the knee and collect in a small sac-like area, creating the cyst.
At The Muscle and Joint Clinic, our chiropractors and physiotherapists assess Baker’s cysts by looking at the knee as a whole. The goal is not only to reduce discomfort behind the knee, but also to understand why the knee is producing excess fluid in the first place. Treatment often focuses on improving knee strength, restoring comfortable movement, reducing irritation, and addressing the mechanical factors that may be contributing to the problem.
What Is a Baker’s Cyst?
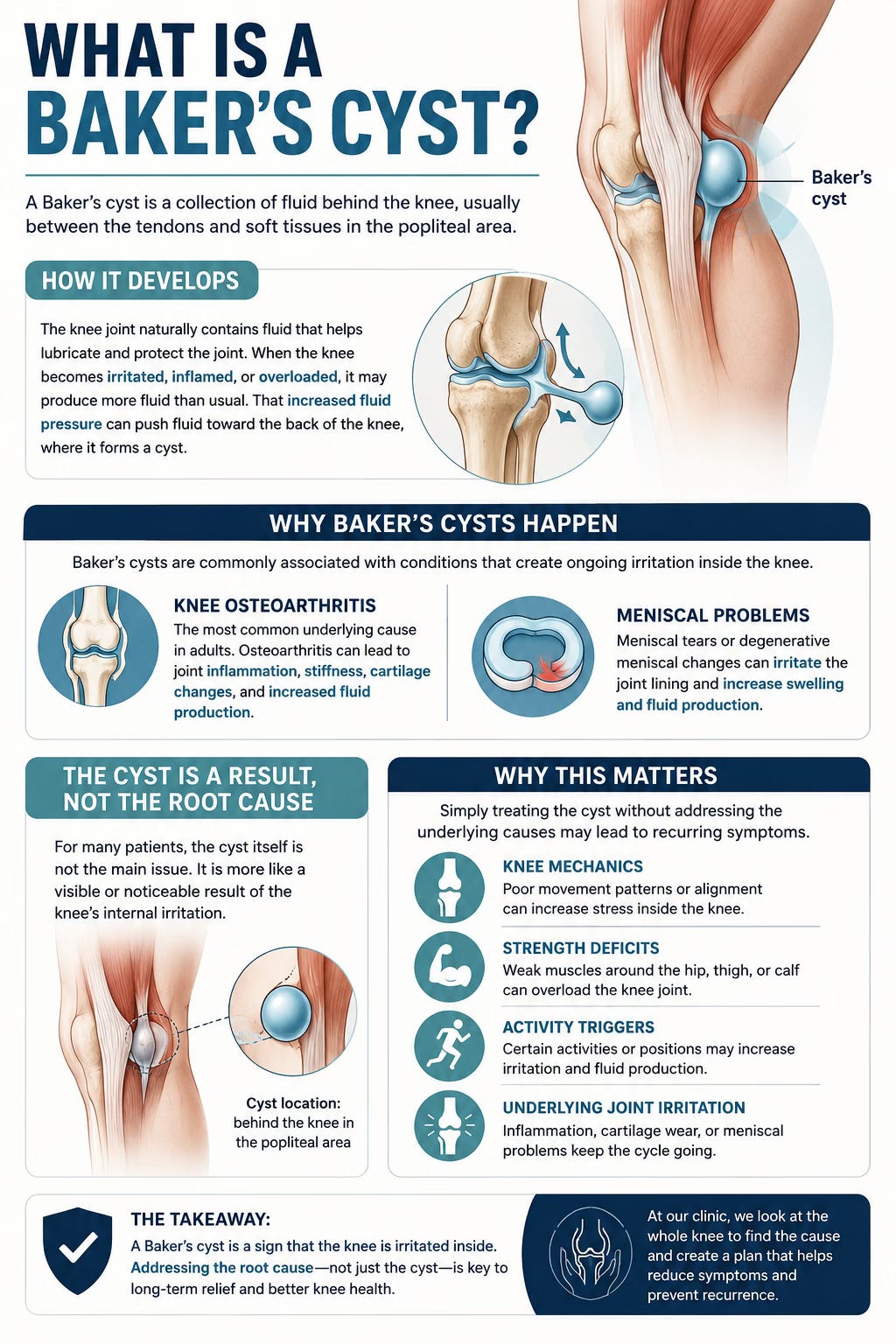
A Baker’s cyst is a collection of fluid behind the knee, usually between the tendons and soft tissues in the popliteal area. The knee joint naturally contains fluid that helps lubricate and protect the joint. When the knee becomes irritated, inflamed, or overloaded, it may produce more fluid than usual. That increased fluid pressure can push fluid toward the back of the knee, where it forms a cyst.
This is why Baker’s cysts are commonly associated with conditions that create ongoing irritation inside the knee. In adults, one of the most common underlying causes is knee osteoarthritis. Osteoarthritis can lead to joint inflammation, stiffness, cartilage changes, and increased fluid production. Meniscal tears or degenerative meniscal changes can also contribute because they may irritate the joint lining and increase swelling.
For some patients, the cyst itself is not the main issue. The cyst is more like a visible or noticeable result of the knee’s internal irritation. This is important because simply treating the cyst without addressing the knee mechanics, strength deficits, activity triggers, or underlying joint irritation may lead to recurring symptoms.
Common Symptoms of a Baker’s Cyst
The symptoms of a Baker’s cyst can vary depending on its size, the level of knee inflammation, and the patient’s activity level. Some people only notice mild swelling behind the knee. Others may feel significant tightness, aching, or restriction.
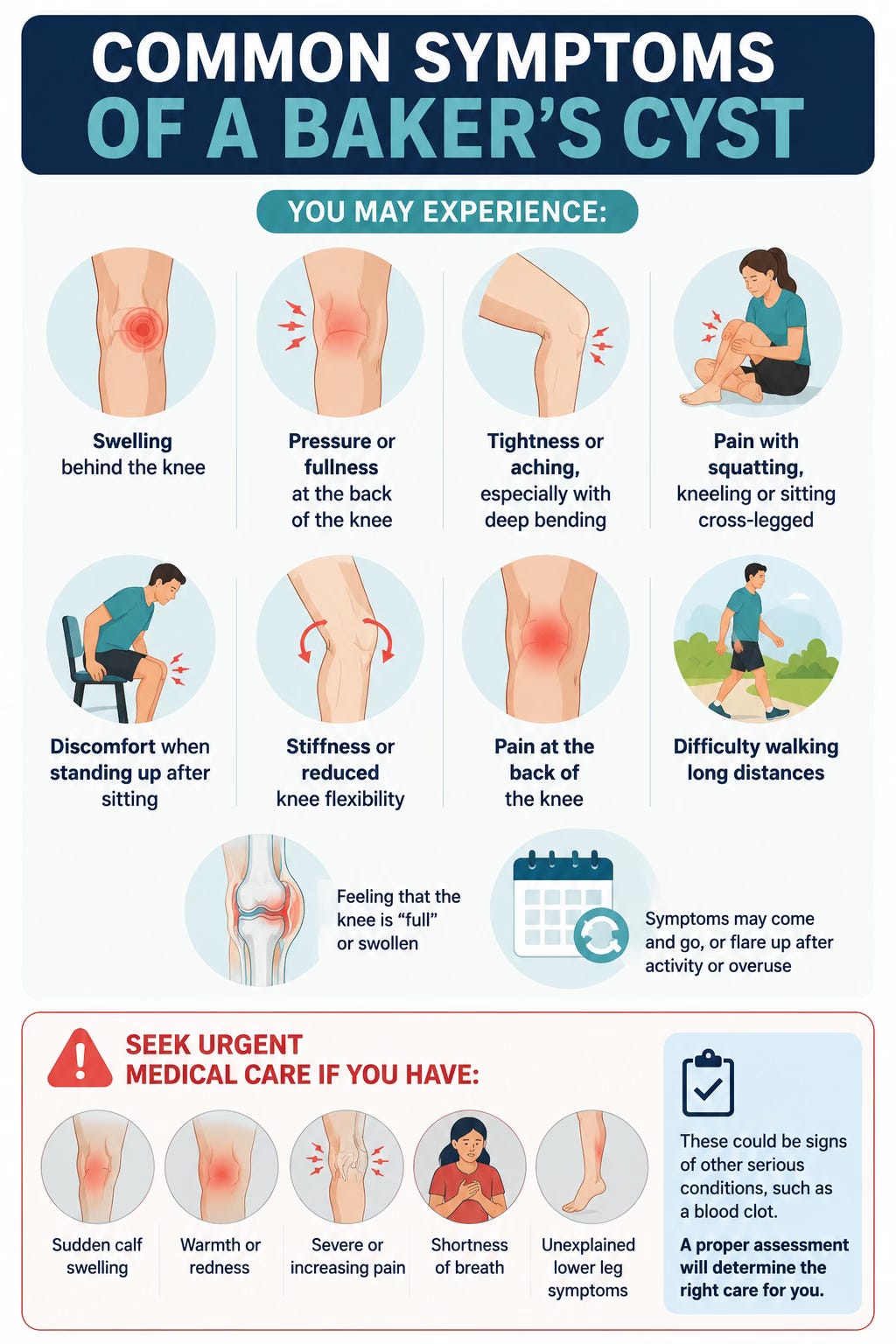
Patients may describe a sensation of pressure at the back of the knee, especially when the knee is fully bent. Sitting cross-legged, kneeling, squatting, or bending the knee deeply may increase symptoms because these positions can raise pressure in the back of the knee. Some people feel discomfort when standing up after sitting for a while, particularly if the knee has been bent for a prolonged period.
Other symptoms may include stiffness, reduced knee flexibility, posterior knee pain, difficulty walking long distances, and a feeling that the knee is “full” or swollen. In some cases, the cyst can fluctuate in size depending on activity levels and inflammation. It may feel more noticeable after prolonged standing, walking, exercise, or a flare-up of knee osteoarthritis.
It is also important to recognize that swelling or pain behind the knee is not always a Baker’s cyst. Sudden calf swelling, warmth, redness, severe pain, shortness of breath, or unexplained lower-leg symptoms should be assessed urgently because other conditions, including a blood clot, can sometimes mimic or overlap with posterior knee symptoms. A proper assessment helps determine whether conservative care is appropriate or whether medical imaging or urgent referral is needed.
Why Baker’s Cysts Happen
A Baker’s cyst usually develops when the knee produces too much joint fluid. This often happens because the knee is reacting to irritation, inflammation, or mechanical stress. The cyst may enlarge when fluid production increases and may decrease when inflammation settles.
Knee osteoarthritis is one of the most common reasons this happens. With osteoarthritis, the joint may become irritated during weight-bearing activity, stairs, squatting, kneeling, or prolonged standing. The body may respond by producing more synovial fluid, leading to swelling inside the knee and sometimes a Baker’s cyst behind it.
Meniscal problems can also contribute. The meniscus acts as a cushion inside the knee. If it becomes torn, irritated, or degenerative, it may create inflammation and swelling. Even when the meniscus is not causing sharp pain, it can still be part of the reason the knee produces extra fluid.
Muscle weakness can also play a role. If the quadriceps, hamstrings, gluteal muscles, or calf muscles are not supporting the knee well, the joint may experience more stress during movement. Poor hip control, limited ankle mobility, altered gait, or foot mechanics may also increase load through the knee. Over time, this can contribute to irritation and swelling.
This is why a Baker’s cyst should be looked at as part of a bigger knee function problem. The treatment plan should not only ask, “How do we shrink the cyst?” It should also ask, “Why is the knee irritated, and what can we do to reduce that irritation?”
The Role of Manual Therapy in Baker’s Cyst Management
Manual therapy can be an important part of conservative Baker’s cyst management, especially when the cyst is associated with knee osteoarthritis or other mechanical knee problems. The strongest rationale for manual therapy is that it targets the underlying drivers of swelling and irritation. Since Baker’s cysts are often linked to excess joint fluid, improving the way the knee moves and tolerates load may help reduce the ongoing irritation that contributes to fluid buildup. The best conservative care is usually not one single modality. Instead, it is a structured plan that combines exercise, education, movement modification, symptom control, and progressive strengthening.
Exercise Is the Foundation of Treatment
Exercise therapy is one of the most important parts of Baker’s cyst rehabilitation because it helps address the knee mechanics and muscle support around the joint. The goal is not to aggressively stretch or force the cyst to disappear. The goal is to improve how the knee handles daily stress so that the joint becomes less irritated over time.
A good rehabilitation program often includes progressive strengthening for the quadriceps, hamstrings, gluteal muscles, and calf muscles. The quadriceps help control knee extension and support the knee during walking, stairs, and sit-to-stand movements. The hamstrings help stabilize the knee and control movement at the back of the thigh. The gluteal muscles, especially the gluteus medius and gluteus maximus, help control hip position and reduce excessive stress through the knee during standing, walking, and stairs. The calf muscles also help with push-off during walking and contribute to lower-limb stability.
For patients with a Baker’s cyst, strengthening usually starts gently. Early exercises may include quad sets, straight leg raises, heel slides, glute bridges, calf raises, and controlled sit-to-stand movements. As symptoms improve, exercises may progress to step-ups, resisted knee extension, hamstring strengthening, hip abduction work, balance exercises, and functional strengthening. The progression should be based on the patient’s pain, swelling, range of motion, and activity goals.
A common mistake is doing too much too soon. If an exercise program causes increased swelling, more pressure behind the knee, or worsening pain that lasts into the next day, the program may need to be adjusted. Baker’s cyst rehabilitation should be progressive, but it should also respect the knee’s irritability.
Why Deep Knee Bending Can Aggravate Symptoms
Many patients with Baker’s cysts notice that symptoms become worse when the knee is deeply bent. This can happen during squatting, kneeling, sitting cross-legged, or crouching. These positions can increase pressure inside the knee and behind the knee, which may make the cyst feel tighter or more uncomfortable.
For this reason, activity modification is often an important part of treatment. Patients may be advised to temporarily reduce prolonged kneeling, deep squatting, high-impact activity, or positions that place the knee in sustained deep flexion. This does not mean the patient must avoid bending the knee forever. Instead, the goal is to calm the knee down first, then gradually restore tolerance to movement as strength and symptoms improve.
In the early stages, range-of-motion exercises are usually kept within a comfortable range. Gentle knee bending and straightening can help maintain mobility without forcing the joint into painful positions. Stationary cycling with low resistance may be useful for some patients, but the bike setup matters. If the seat is too low, the knee bends too much and may increase posterior knee pressure. Adjusting the seat height can often make cycling more comfortable.
Manual Therapy and Chiropractic Care
Chiropractic care can support Baker’s cyst management by addressing joint mechanics, soft tissue restriction, and movement patterns that may be contributing to knee stress. At The Muscle and Joint Clinic, our chiropractors do not look only at the cyst. They assess the knee, hip, ankle, foot, gait pattern, and the way the patient moves during functional tasks.
For example, limited ankle mobility may change how a patient squats, walks, or goes down stairs. Weak hip control may cause the knee to collapse inward during movement. Foot mechanics may affect how load travels through the lower limb. Hip stiffness may alter stride and increase compensatory stress at the knee. These factors can all contribute to irritation in an already sensitive knee.
Chiropractic treatment may include soft tissue therapy, joint mobilization, stretching, movement coaching, and exercise prescription. In some cases, chiropractic adjustments or mobilizations may be used for the hip, ankle, foot, or spine if those areas are contributing to altered mechanics. The treatment is individualized based on the patient’s assessment findings and comfort level.
Manual therapy may help reduce stiffness and improve short-term movement quality, but it is usually most effective when paired with exercise. Hands-on care may help a patient move more comfortably, while strengthening helps maintain better function over time.
Modalities can be useful for symptom management, especially during painful or swollen phases. However, modalities should usually be viewed as supportive tools rather than the entire treatment plan.
Ice or cold therapy may be helpful when the knee feels irritated, swollen, or inflamed. It can be used after activity or exercise to help manage discomfort. Compression sleeves or elastic wraps may also help some patients feel more supported and may assist with swelling control.
Electrical stimulation, such as TENS or IFC, may help reduce pain sensitivity and allow the patient to participate more comfortably in rehabilitation. Therapeutic ultrasound may be used in some settings, although evidence for directly reducing Baker’s cyst size is limited. These approaches can help with comfort, but they do not replace the need to address strength, movement, activity tolerance, and the underlying knee condition.
This distinction is important. A patient may feel temporary relief after a modality, but if the knee remains weak, overloaded, stiff, or irritated, the cyst may continue to be symptomatic. The best conservative plans usually combine short-term symptom relief with long-term functional improvement.
When Aspiration or Injection May Be Considered
Some Baker’s cysts improve with conservative care. Others remain painful, large, or limiting despite rehabilitation. In those situations, referral for medical assessment may be appropriate. Ultrasound-guided aspiration and corticosteroid injection are sometimes used when a cyst is persistently symptomatic.
Aspiration involves removing fluid from the cyst, usually under ultrasound guidance. Corticosteroid injection may be used to reduce inflammation. Research suggests that aspiration and injection can reduce cyst size and symptoms in many patients, although recurrence can occur, especially if the underlying knee problem continues to produce excess fluid.
One randomized controlled trial compared ultrasound-guided aspiration and corticosteroid injection, horizontal therapy, and a combination of both in patients with knee osteoarthritis and Baker’s cysts. The combined approach showed the best outcomes for pain, function, and cyst size reduction. This supports a practical clinical point: when a cyst is large or persistent, medical procedures may help reduce the fluid collection, but rehabilitation remains important because the knee still needs to be strengthened and managed properly.
At The Muscle and Joint Clinic, if a patient’s presentation suggests that imaging, aspiration, injection, or specialist referral may be needed, we can recommend appropriate next steps and communicate with the patient’s medical provider.
The Importance of Imaging
A Baker’s cyst can often be suspected based on the patient’s symptoms and a physical examination, but imaging may be helpful in many cases. Ultrasound is commonly used because it can confirm the presence of a cyst, measure its size, and help assess whether other causes of swelling may be present.
Imaging is especially useful when the swelling is large, symptoms are worsening, the diagnosis is uncertain, or the patient has calf symptoms. It can also help guide medical procedures such as aspiration or injection.
In some cases, MRI may be recommended if there is suspicion of meniscal injury, ligament injury, cartilage damage, or other internal knee pathology. Since Baker’s cysts are often linked to problems inside the knee, identifying the underlying cause can help guide treatment more effectively.
What Patients Can Do at Home
Home care can make a meaningful difference when it is done properly. Patients are often encouraged to avoid positions that clearly aggravate symptoms, such as prolonged deep squatting, kneeling, or sitting cross-legged. Gentle walking may be helpful if it does not increase swelling. Low-impact exercise is often better tolerated than high-impact activity during flare-ups.
Using ice after activity may help reduce irritation. Compression may provide support and help manage swelling. Elevating the leg can be useful if there is generalized knee swelling. However, patients should avoid aggressively massaging the cyst or trying to “break it up,” as this may irritate the area.
Exercise should be specific and progressive. Random stretching or heavy strengthening may not be appropriate in the early stages. A guided plan from a chiropractor or physiotherapist can help ensure the patient is doing the right exercises at the right intensity.
How The Muscle and Joint Clinic Assesses Baker’s Cysts
At The Muscle and Joint Clinic, assessment begins with a detailed history. We ask when the swelling started, what movements make it worse, whether there was a specific injury, whether the patient has known arthritis or meniscal issues, and whether the symptoms are changing. We also ask about calf pain, redness, warmth, numbness, instability, locking, or other symptoms that may require referral.
The physical examination may include checking knee range of motion, swelling, tenderness, strength, walking pattern, squat mechanics, stair mechanics, hip control, ankle mobility, and functional tolerance. We also assess whether the symptoms appear to be coming mainly from the cyst, the knee joint, surrounding muscles, or another structure.
This assessment helps determine whether conservative care is appropriate and what type of treatment plan is most likely to help. For some patients, the focus may be swelling control and gentle mobility. For others, the main need may be strengthening and movement retraining. For patients with suspected osteoarthritis or meniscal involvement, the plan may include education on long-term knee management.

How Our Chiropractors and Physiotherapists Treat Baker’s Cyst-Related Knee Pain
Treatment at The Muscle and Joint Clinic is individualized. Our chiropractors and physiotherapists may use a combination of hands-on care, exercise rehabilitation, education, modalities, and activity modification.
In the early stage, the focus may be reducing pain and calming the knee. This can include gentle soft tissue therapy, knee or lower-limb mobilization, swelling management, compression advice, and low-load exercises. Patients are taught which activities to avoid temporarily and which movements are safe to continue.
As symptoms improve, the plan usually shifts toward progressive strengthening. The patient may work on quadriceps strength, hamstring control, glute strength, calf strength, balance, and functional movement patterns. The goal is to help the knee tolerate daily tasks with less irritation.
Later-stage care may include return-to-activity planning. This may involve stairs, squatting modifications, walking tolerance, work-specific tasks, sport-specific movements, or exercise progressions. If the patient has knee osteoarthritis, the plan may also include long-term strategies to manage flare-ups and maintain strength.
The key is that treatment should not be passive only. A Baker’s cyst often reflects an irritated knee joint, and long-term improvement usually requires better joint support and better load management.
When to Seek Care
A person should consider an assessment if they have swelling behind the knee, recurring tightness, pain with bending, difficulty standing after sitting, or discomfort with walking, stairs, squatting, or kneeling. Early assessment can help identify whether the issue is likely a Baker’s cyst and whether the knee is showing signs of osteoarthritis, meniscal irritation, or another problem.
Urgent medical assessment is recommended if there is sudden calf swelling, redness, warmth, severe pain, shortness of breath, chest pain, or unexplained worsening of symptoms. These symptoms may indicate something more serious and should not be treated as a simple Baker’s cyst without medical evaluation.
The Key Takeaway
A Baker’s cyst is often a sign that the knee is irritated and producing excess fluid. While the swelling is located behind the knee, the underlying cause may involve knee osteoarthritis, meniscal irritation, joint inflammation, muscle weakness, altered mechanics, or previous injury.
Physiotherapy and chiropractic care can help by improving strength, restoring mobility, reducing mechanical stress, managing symptoms, and addressing the factors that may be contributing to excess joint fluid. Modalities such as ice, IFC, TENS, ultrasound, or compression may help with pain and swelling, but the foundation of treatment is usually a structured exercise and movement plan.
At The Muscle and Joint Clinic, our chiropractors and physiotherapists work together to assess the knee, identify contributing factors, provide hands-on care, guide rehabilitation, and recommend imaging or referral when needed.
If you have swelling, tightness, or pain behind the knee, a proper assessment can help determine whether a Baker’s cyst may be involved and what treatment approach is best for you.
Book a free consultation at The Muscle and Joint Clinic to learn how our chiropractors and physiotherapists can help with Baker’s cyst-related knee pain and stiffness.
References
Ionescu, E. V., Stanciu, L. E., Bujduveanu, A., et al. (2023). Clinical evidence regarding the dynamic of Baker cyst dimensions after intermittent vacuum therapy as rehabilitation treatment in patients with knee osteoarthritis. Journal of Clinical Medicine.
Van Nest, D. S., Tjoumakaris, F. P., Smith, B. J., Beatty, T. M., & Freedman, K. B. (2020). Popliteal cysts: A systematic review of nonoperative and operative treatment. JBJS Reviews.
Herman, A. M., & Marzo, J. M. (2014). Popliteal cysts: A current review. Orthopedics.
Di Sante, L., Paoloni, M., Dimaggio, M., et al. (2012). Ultrasound-guided aspiration and corticosteroid injection compared to horizontal therapy for treatment of knee osteoarthritis complicated with Baker’s cyst: A randomized, controlled trial. European Journal of Physical and Rehabilitation Medicine.
Deyle, G. D., Allen, C. S., Allison, S. C., et al. (2020). Physical therapy versus glucocorticoid injection for osteoarthritis of the knee. The New England Journal of Medicine.
Sharma, L. (2021). Osteoarthritis of the knee. The New England Journal of Medicine.
Katz, J. N., Collins, J. E., Bisson, L., et al. (2025). A randomized trial of physical therapy for meniscal tear and knee pain. The New England Journal of Medicine.
Logan, C. A., Asnis, P. D., & Provencher, M. T. (2017). The role of therapeutic modalities in surgical and nonsurgical management of orthopaedic injuries. Journal of the American Academy of Orthopaedic Surgeons.
da Silva, A. N. G., de Oliveira, J. R. S., Madureira, Á. N. M., Lima, W. A., & Lima, V. L. M. (2022). Biochemical and physiological events involved in responses to the ultrasound used in physiotherapy: A review. Ultrasound in Medicine & Biology.
French, H. P., Abbott, J. H., & Galvin, R. (2022). Adjunctive therapies in addition to land-based exercise therapy for osteoarthritis of the hip or knee. Cochrane Database of Systematic Reviews.
American Academy of Orthopaedic Surgeons. (2021). Management of osteoarthritis of the knee: Evidence-based clinical practice guideline.
Department of Veterans Affairs. (2020). The non-surgical management of hip and knee osteoarthritis.
Curl, W. W. (1996). Popliteal cysts: Historical background and current knowledge. Journal of the American Academy of Orthopaedic Surgeons.
Smith, M. K., Lesniak, B., Baraga, M. G., Kaplan, L., & Jose, J. (2015). Treatment of popliteal Baker cysts with ultrasound-guided aspiration, fenestration, and injection: Long-term follow-up. Sports Health.