
Chiropractic Care During Pregnancy
Supporting Pain Relief, Movement, Exercise, and Postpartum Recovery


Pregnancy is one of the most significant physical changes a person can experience. As the body adapts to support a growing baby, nearly every part of the musculoskeletal system is affected in some way. The spine, pelvis, hips, ribs, abdominal wall, pelvic floor, muscles, ligaments, and joints all respond to changing weight distribution, hormonal changes, altered posture, and new daily demands.
For many people, these changes are manageable. For others, they can contribute to low back pain, pelvic girdle pain, hip discomfort, rib pain, neck tension, headaches, difficulty sleeping, or trouble with everyday activities such as walking, climbing stairs, rolling in bed, sitting, standing, lifting, or caring for other children.
These symptoms are common, but they should not be dismissed as “just part of pregnancy.” Pregnancy-related low back pain and pelvic girdle pain can affect sleep, work, activity levels, mood, confidence with movement, and quality of life. Research has reported that low back pain, pelvic girdle pain, or a combination of both are frequently experienced during pregnancy, and some individuals continue to experience symptoms into the postpartum period (Weis et al., 2020; Weis et al., 2022).
Chiropractic care during pregnancy is not about “treating pregnancy.” Pregnancy is not a disease. Instead, chiropractic care focuses on the musculoskeletal system: the spine, pelvis, joints, muscles, nerves, movement patterns, and daily function. The goal is to help patients understand what is changing, manage discomfort where appropriate, move more comfortably, stay active when safe, and transition into postpartum recovery with more confidence.
The Canadian Chiropractic Association has highlighted several reasons why a pregnant person may consider chiropractic care, including education, pain relief, guidance around physical activity, postpartum support, and ergonomic advice for feeding and infant care (Canadian Chiropractic Association [CCA], 2026). These themes are also reflected in the best-practice recommendations for chiropractic care for pregnant and postpartum patients with low back pain, pelvic girdle pain, or combined pain (Weis et al., 2022).
Why Pregnancy Can Affect the Spine and Pelvis
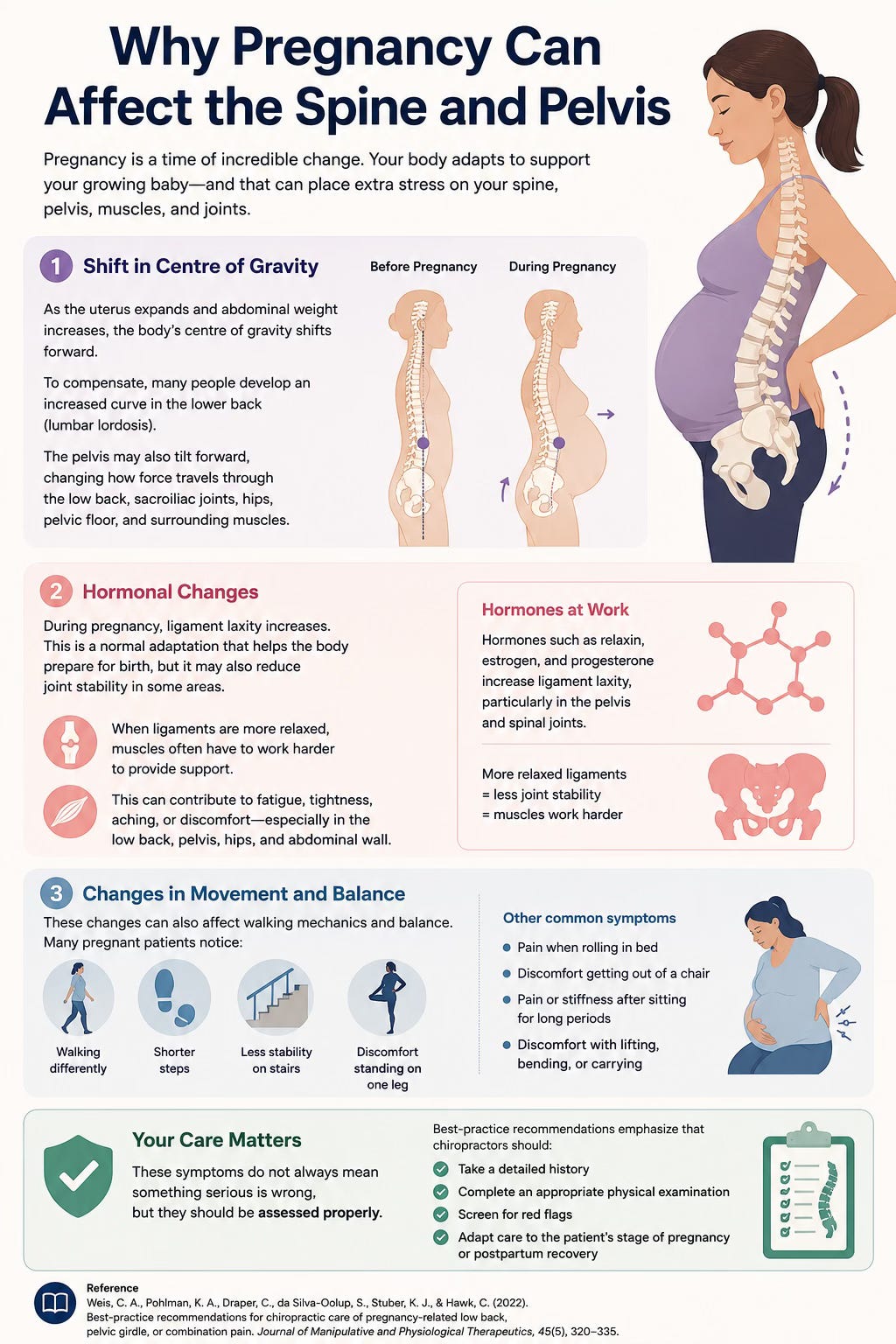
During pregnancy, the body changes in ways that can affect posture, balance, and movement. As the uterus expands and abdominal weight increases, the body’s centre of gravity often shifts forward. To compensate, many people develop an increased curve in the lower back, known as lumbar lordosis. The pelvis may also tilt forward, changing the way force travels through the low back, sacroiliac joints, hips, pelvic floor, and surrounding muscles.
Hormonal changes also play a role. During pregnancy, ligament laxity increases. This is a normal adaptation that helps the body prepare for birth, but it may also reduce joint stability in some areas. When ligaments are more relaxed, muscles often have to work harder to provide support. This can contribute to fatigue, tightness, aching, or discomfort, especially in the low back, pelvis, hips, and abdominal wall.
These changes can also affect walking mechanics and balance. Some pregnant patients notice they walk differently, take shorter steps, feel less stable on stairs, or have discomfort when standing on one leg. Others may experience pain when rolling in bed, getting out of a chair, sitting for long periods, or lifting.
These symptoms do not always mean something serious is wrong, but they should be assessed properly. Best-practice recommendations emphasize that chiropractors should take a detailed history, complete an appropriate physical examination, screen for red flags, and adapt care to the patient’s stage of pregnancy or postpartum recovery (Weis et al., 2022).
Low Back Pain and Pelvic Girdle Pain Are Not the Same Thing
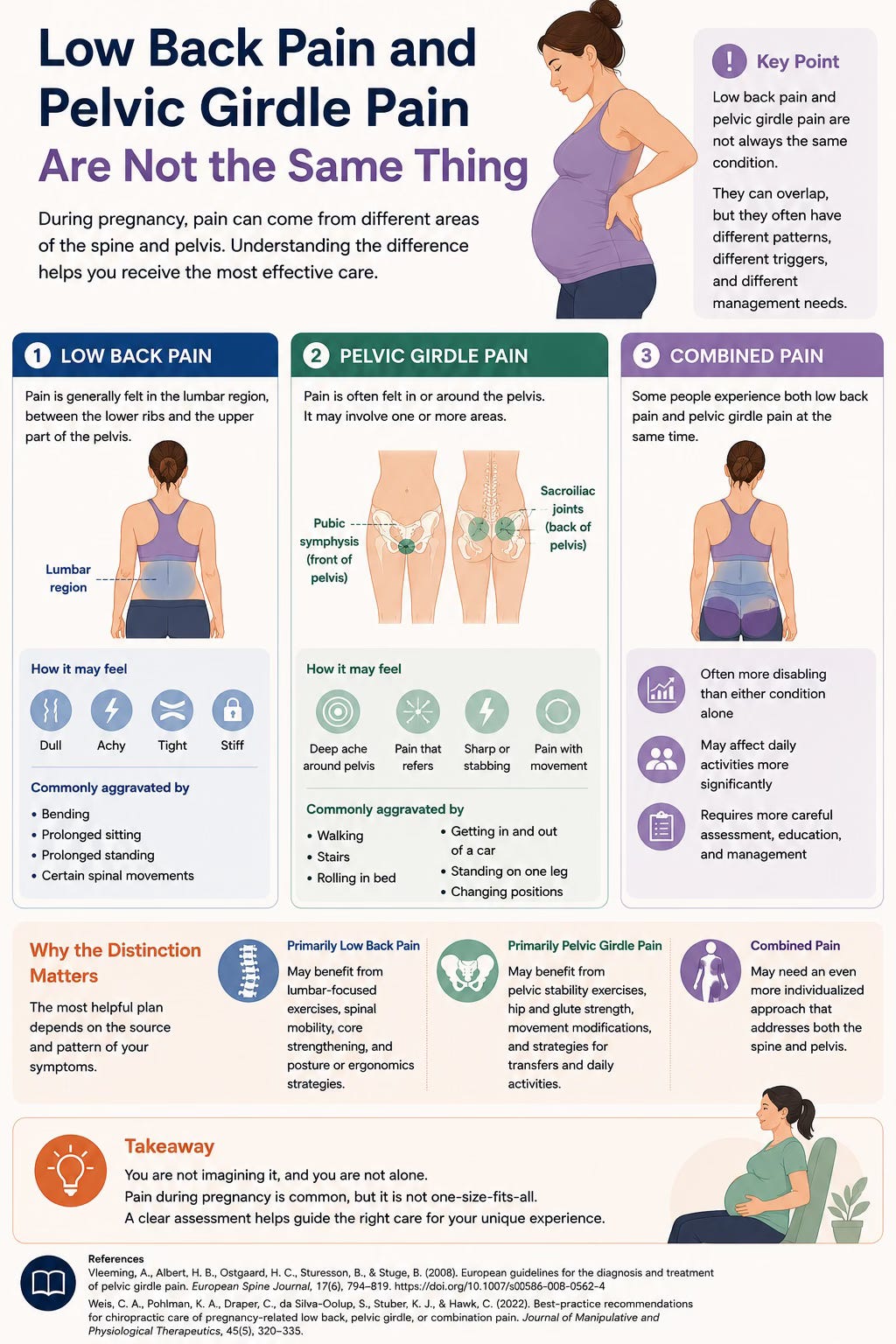
One of the most important points in the pregnancy-related pain literature is that low back pain and pelvic girdle pain are not always the same condition. They can overlap, but they often have different patterns, different aggravating factors, and different management needs.
Low back pain is generally described as pain in the lumbar region, between the lower ribs and the upper part of the pelvis. It may feel dull, achy, tight, or stiff. It may be aggravated by bending, prolonged sitting, prolonged standing, or certain spinal movements (Weis et al., 2022).
Pelvic girdle pain is different. It is often felt near the sacroiliac joints at the back of the pelvis, the pubic symphysis at the front of the pelvis, or both. It may refer into the buttock or posterior thigh. Pelvic girdle pain may be aggravated by walking, stairs, rolling in bed, getting in and out of a car, standing on one leg, or changing positions (Vleeming et al., 2008; Weis et al., 2022).
Some patients experience both low back pain and pelvic girdle pain at the same time. This is often called combined pain. Combined pain may be more disabling than low back pain or pelvic girdle pain alone, and patients with combined pain may require more careful assessment, education, and management (Weis et al., 2022).
This distinction matters because the most helpful plan depends on the source and pattern of symptoms. A patient with primarily lumbar pain may benefit from different exercises, manual therapy, and ergonomic strategies than a patient with pelvic girdle pain. A patient with combined pain may need an even more individualized approach.
Pain During Pregnancy Should Not Be Ignored
A common misconception is that back or pelvic pain during pregnancy is unavoidable and should simply be tolerated until delivery. While many pregnancy-related symptoms improve after birth, some patients continue to experience pain postpartum. The 2020 systematic review by Weis and colleagues noted that pregnancy-related low back pain or pelvic girdle pain can interfere with activities of daily living and may lead some patients to delay care because they believe the pain is a normal part of pregnancy (Weis et al., 2020).
This is important because delayed care may allow symptoms to become more persistent. Some patients continue to experience low back or pelvic symptoms months or even years postpartum, especially if they had significant symptoms during pregnancy or combined pain patterns (Weis et al., 2022).
Seeking care does not mean the pregnancy is abnormal. It means the patient is looking for support to move better, function better, and manage symptoms in a safe and appropriate way.

What Does the Research Say About Chiropractic Care During Pregnancy?
A 2020 systematic review examined chiropractic care options commonly used for pregnancy-related low back pain, pelvic girdle pain, or combination pain. The review included 50 articles from 18 systematic reviews, 30 randomized controlled trials, and 2 cohort studies (Weis et al., 2020).
The review found several interventions with favorable or potentially useful evidence. For pregnancy-related low back pain, electrotherapy and osteopathic manipulative therapy had moderate favorable evidence. Chiropractic care, exercise, and support devices had inconclusive but favorable evidence. (Weis et al., 2020). For pregnancy-related pelvic girdle pain, exercise had favorable evidence. (Weis et al., 2020).
For patients with low back pain or pelvic girdle pain, multimodal care, patient education, and physiotherapy had favorable evidence. Exercise had moderate evidence, with some positive findings (Weis et al., 2020).
The main takeaway is not that one single treatment is clearly superior for every pregnant patient. The better takeaway is that pregnancy-related back and pelvic pain should be assessed individually, and care is often best delivered as a combination of education, exercise, manual therapy where appropriate, ergonomic advice, support strategies, and collaboration with prenatal healthcare providers.
Why Multimodal Care Matters
In clinical practice, chiropractic care is rarely just one thing. It is usually multimodal, meaning it may include several components. This may involve patient education, advice on daily activities, spinal or pelvic joint mobilization, soft tissue therapy, exercise prescription, support belts, taping, pillow positioning, and home-care strategies.
This multimodal approach is important because pregnancy-related pain is often multifactorial. Pain may be influenced by posture, joint loading, muscle endurance, sleep position, activity level, pelvic stability, abdominal wall changes, work demands, and previous injury history. It would be unrealistic to expect one technique alone to solve every case.
The 2020 systematic review found favorable evidence for multimodal care in patients with low back pain or pelvic girdle pain during pregnancy (Weis et al., 2020). One randomized trial included in the review compared usual obstetric care with a multimodal program that included manual therapy, exercise, and education. The multimodal group had improvements in pain and disability compared with usual obstetric care alone when applied between 24 and 33 weeks of gestation (George et al., 2013, as cited in Weis et al., 2020).
This supports what many clinicians see in practice: patients often do best when care includes both symptom relief and active strategies to improve function.
Education Is a Key Part of Pregnancy Care
Education is one of the most valuable parts of chiropractic care during pregnancy. Many patients are unsure which symptoms are common, which symptoms require medical attention, and how to safely modify their daily activities.
A chiropractor can help explain how pregnancy-related physical changes may affect posture, joint loading, muscle function, movement patterns, and pain. Education may include advice about sleeping positions, pillow support, workstation setup, lifting mechanics, footwear, walking tolerance, exercise modifications, and pacing daily activities.
Best-practice recommendations emphasize that pregnant and postpartum patients should be encouraged to take an active role in their care. They should receive information about anatomy, biomechanics, controlled movement patterns, and strategies to continue daily activities as tolerated (Weis et al., 2022).
This matters because fear can lead to unnecessary inactivity. Some pregnant patients stop moving because they worry that exercise or daily activity will worsen their pain or harm the pregnancy. However, in the absence of contraindications, physical activity during pregnancy is recommended and is associated with several maternal and fetal health benefits (Mottola et al., 2018).
Physical Activity During Pregnancy: What the Canadian Guideline Recommends
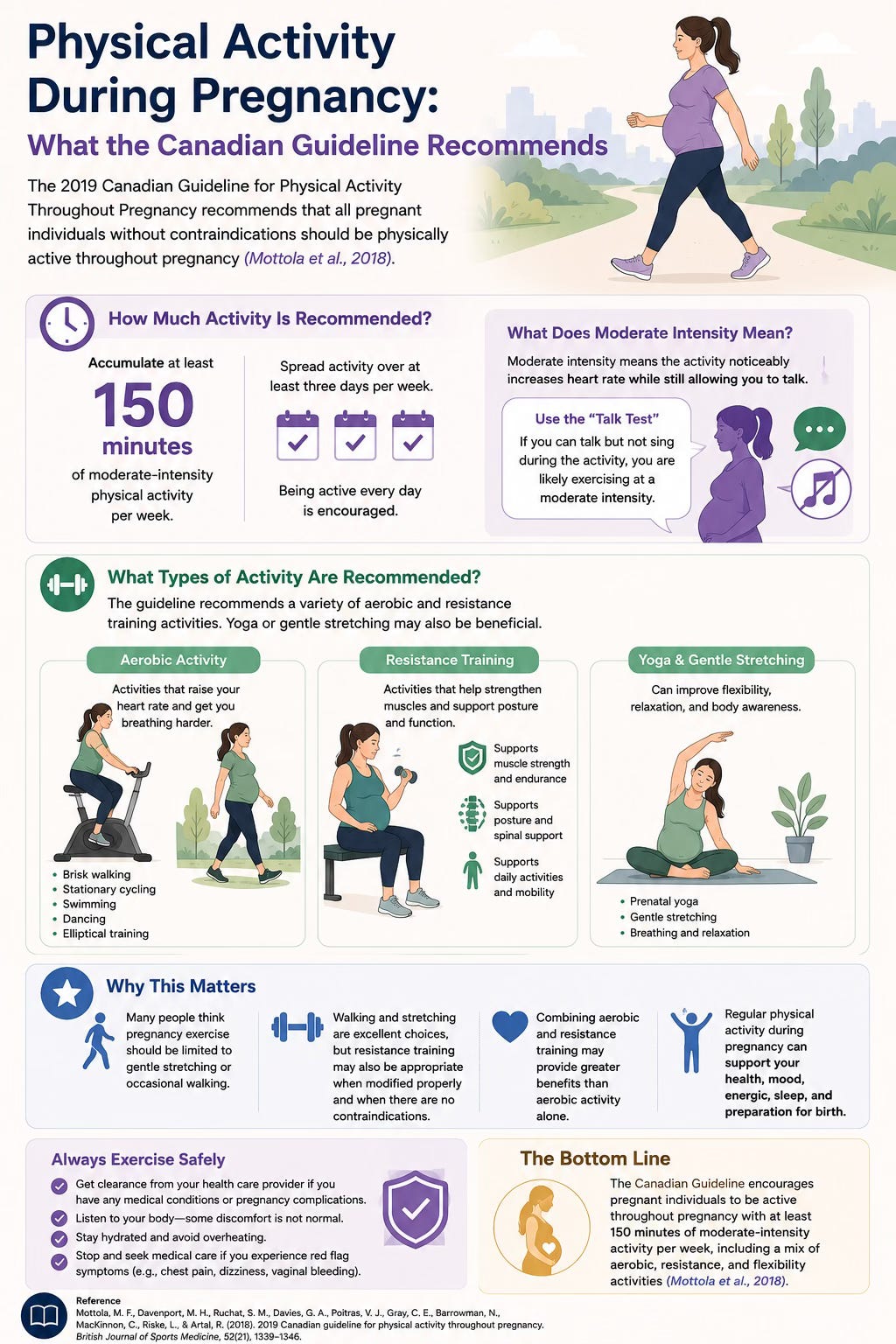
The 2019 Canadian Guideline for Physical Activity Throughout Pregnancy recommends that all pregnant individuals without contraindications should be physically active throughout pregnancy (Mottola et al., 2018).
The guideline recommends accumulating at least 150 minutes of moderate-intensity physical activity per week. Moderate intensity means the activity noticeably increases heart rate while still allowing the person to talk. This is often described using the “talk test.” If a person can talk but not sing during the activity, they are likely exercising at a moderate intensity.
The guideline also recommends that activity be spread over at least three days per week, although being active every day is encouraged. It recommends a variety of aerobic and resistance training activities, and notes that yoga or gentle stretching may also be beneficial (Mottola et al., 2018).
This is important because many people assume pregnancy exercise should be limited to gentle stretching or occasional walking. While walking and stretching can be excellent, resistance training may also be appropriate when modified properly and when there are no contraindications. Combining aerobic and resistance training may provide greater benefits than aerobic activity alone (Mottola et al., 2018).
The Health Benefits of Prenatal Physical Activity
The Canadian guideline describes prenatal physical activity as a front-line therapy for reducing pregnancy complications and improving maternal physical and mental health (Mottola et al., 2018).
According to the guideline, prenatal physical activity is associated with decreased risk of preeclampsia, gestational hypertension, gestational diabetes, caesarean section, instrumental delivery, urinary incontinence, excessive gestational weight gain, and depression. It is also associated with improved blood glucose, decreased total gestational weight gain, reduced depressive symptom severity, and decreased severity of lumbopelvic pain (Mottola et al., 2018).
The guideline also addresses common safety concerns. In women without contraindications, physical activity during pregnancy was not associated with miscarriage, stillbirth, neonatal death, preterm birth, preterm or prelabour rupture of membranes, neonatal hypoglycemia, low birth weight, birth defects, induction of labour, or birth complications (Mottola et al., 2018).
This does not mean every activity is appropriate for every pregnant person. It means movement should be encouraged, modified when needed, and individualized based on symptoms, pregnancy stage, health history, and obstetric guidance.
Exercise and Pregnancy-Related Back or Pelvic Pain
Exercise can be an important part of managing pregnancy-related low back pain and pelvic girdle pain. The Canadian guideline reported that prenatal physical activity can reduce the severity of lumbopelvic pain (Mottola et al., 2018). Best-practice chiropractic recommendations also encourage pregnant patients with low back pain or pelvic girdle pain to remain active where possible, continue normal activities as tolerated, and follow an individualized exercise program (Weis et al., 2022).
The 2020 systematic review found that exercise had favorable evidence for pregnancy-related low back pain and pelvic girdle pain, although results varied depending on the type of pain, exercise program, study quality, and dosage (Weis et al., 2020).
This is why exercise should be individualized. A person with mild low back stiffness may tolerate general walking, mobility work, and strengthening quite well. A person with significant pelvic girdle pain may need more careful exercise selection because certain movements, such as wide stances, stairs, single-leg loading, or uneven walking, can aggravate symptoms.
For some patients, a supervised or guided program may be helpful. Exercises may include hip strengthening, glute activation, gentle core coordination, pelvic floor muscle training, breathing strategies, mobility exercises, and postural endurance work. The goal is not to overload the patient. The goal is to help them move with more confidence and less irritation.
Previously Inactive Patients Can Still Start
One of the most helpful parts of the Canadian guideline is that it does not only apply to people who were active before pregnancy. The guideline specifically states that previously inactive women without contraindications should also be physically active throughout pregnancy (Mottola et al., 2018).
This is important because some people believe pregnancy is not the time to start exercising. While pregnancy may not be the time to suddenly begin intense or unfamiliar training, it can be an appropriate time to gradually introduce safe physical activity.
Previously inactive patients may need to begin with lower intensity, shorter duration, and slower progression. This may include short walks, gentle mobility, breathing exercises, pelvic floor awareness, and basic strengthening. Over time, activity can be increased based on tolerance, symptoms, fatigue, and medical guidance.
The goal is not perfection. The goal is progress.
Pelvic Floor Muscle Training
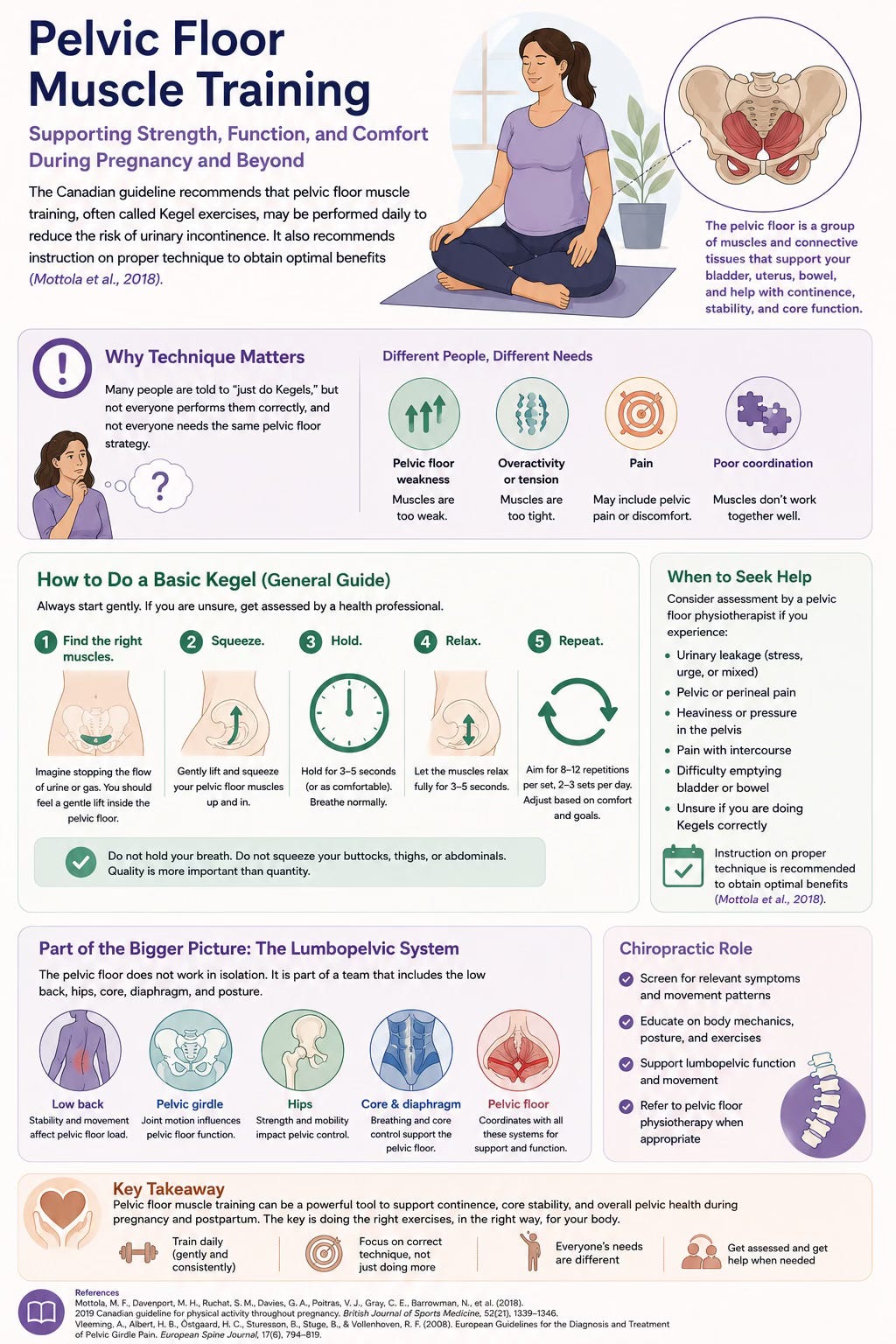
The Canadian guideline recommends that pelvic floor muscle training, often called Kegel exercises, may be performed daily to reduce the risk of urinary incontinence. It also recommends instruction on proper technique to obtain optimal benefits (Mottola et al., 2018).
This is important because many people are told to “just do Kegels,” but not everyone performs them correctly, and not everyone needs the same pelvic floor strategy. Some patients may have pelvic floor weakness, while others may have overactivity, tension, pain, or poor coordination.
For chiropractic care, pelvic floor considerations are relevant because the pelvic floor is part of the broader lumbopelvic system. Low back pain, pelvic girdle pain, hip function, breathing mechanics, abdominal wall control, and pelvic floor coordination can all interact. Chiropractors can screen, educate, and refer to pelvic floor physiotherapy when appropriate.
Manual Therapy During Pregnancy
Manual therapy can be one part of care for pregnancy-related low back or pelvic pain. Depending on the patient, this may include spinal manipulation, mobilization, soft tissue therapy, gentle stretching, or other hands-on techniques.
Best-practice recommendations state that spinal manipulative therapy may be appropriate for some pregnant and postpartum patients with low back pain, pelvic girdle pain, or combined pain, while also emphasizing the need for modifications, informed consent, and attention to contraindications (Weis et al., 2022).
Care should be individualized. Some patients may benefit from gentle mobilization, soft tissue therapy, low-force approaches, or modified adjusting techniques. Others may respond better to exercise, education, support belts, or co-management with physiotherapy, pelvic floor physiotherapy, massage therapy, midwifery, or obstetric care.
The treatment should fit the patient, not the other way around.
Support Belts, Pillows, Taping, and Home Strategies
Many patients benefit from simple supportive strategies during pregnancy. Pillow support can help with sleep positioning. A pillow between the knees, under the abdomen, or supporting the back may reduce strain and improve comfort. Best-practice recommendations note that pregnant patients may consider pillow support under the abdomen, legs, or knees to help manage pregnancy-related back pain and sleep discomfort (Weis et al., 2022).
Support belts may provide short-term symptomatic relief for some patients with low back pain, pelvic girdle pain, or combined pain. The 2020 systematic review found that support devices had inconclusive evidence, but some studies showed favorable findings for pain relief or improved function with certain activities (Weis et al., 2020). Best-practice recommendations suggest that pelvic belts may be considered for short periods of symptomatic relief, especially when combined with education and exercise (Weis et al., 2022).
Taping may also be considered in some cases. However, clinicians should check for skin sensitivity or adhesive reactions. If irritation occurs, the tape should be removed and not reapplied (Weis et al., 2022).
These tools are not cures, but they can help patients function better while they continue working on movement, strength, and recovery.
Supine Exercise and Position Modifications
The Canadian guideline recommends that pregnant individuals who feel light-headed, nauseous, or unwell when exercising flat on their back should modify their position to avoid the supine position (Mottola et al., 2018).
Some pregnant patients feel uncomfortable lying flat on their back, especially later in pregnancy. They may experience dizziness, nausea, shortness of breath, or a feeling of pressure. In these cases, exercises can often be modified to side-lying, seated, standing, quadruped, or inclined positions.
This is also relevant during chiropractic treatment. Care should be modified for comfort and safety. Side-lying positions, pillows, pregnancy cushions, seated techniques, and lower-force approaches may all be used depending on the patient.
Safety: When Exercise Should Stop
The Canadian guideline provides clear reasons to stop physical activity and consult a healthcare provider. These include persistent excessive shortness of breath that does not resolve with rest, severe chest pain, regular and painful uterine contractions, vaginal bleeding, persistent loss of fluid from the vagina, and persistent dizziness or faintness that does not resolve with rest (Mottola et al., 2018).
These symptoms should not be ignored. They are not typical exercise discomforts and require medical guidance.
The guideline also lists absolute contraindications to exercise, including ruptured membranes, premature labour, unexplained persistent vaginal bleeding, placenta previa after 28 weeks, preeclampsia, incompetent cervix, intrauterine growth restriction, high-order multiple pregnancy, uncontrolled type 1 diabetes, uncontrolled hypertension, uncontrolled thyroid disease, and other serious cardiovascular, respiratory, or systemic disorders (Mottola et al., 2018).
Relative contraindications include recurrent pregnancy loss, gestational hypertension, history of spontaneous preterm birth, mild or moderate cardiovascular or respiratory disease, symptomatic anemia, malnutrition, eating disorder, twin pregnancy after 28 weeks, and other significant medical conditions (Mottola et al., 2018). Patients with relative contraindications should discuss physical activity with their obstetric care provider.
Chiropractic Care and Red Flags
Best-practice chiropractic recommendations also highlight the importance of red flag screening. Certain symptoms or conditions may require medical clearance, treatment modification, referral, or co-management.
Caution is recommended with vaginal bleeding without prior clearance, abdominopelvic cramping, ruptured membranes, premature labour, placenta previa with bleeding, placenta abruption, ectopic pregnancy concerns, bowel obstruction, pregnancy-induced hypertension, preeclampsia, eclampsia, recent pelvic trauma, known bleeding disorders, and other high-risk situations (Weis et al., 2022).
Blood pressure is particularly important. Hypertensive disorders of pregnancy can develop quickly and may also occur postpartum. Best-practice recommendations advise blood pressure monitoring during pregnancy and postpartum in appropriate circumstances, and immediate referral when concerning findings are present (Weis et al., 2022).
This reinforces an important point: chiropractic care during pregnancy should be careful, informed, and collaborative. It should support prenatal care, not replace it.
Diastasis Recti and Abdominal Wall Recovery
During pregnancy, the abdominal wall stretches as the uterus grows. Many patients develop some degree of increased separation between the rectus abdominis muscles, commonly referred to as diastasis recti. This occurs because the linea alba, the connective tissue between the abdominal muscles, stretches and thins.
Best-practice recommendations suggest that pregnant and postpartum patients should be checked for diastasis recti where appropriate (Weis et al., 2022). The Canadian physical activity guideline also notes that people with diastasis recti should seek physiotherapy advice and avoid abdominal strengthening exercises such as abdominal curls if those exercises worsen the condition (Mottola et al., 2018).
This does not mean the core should never be trained during or after pregnancy. It means the approach should be appropriate. Good rehabilitation should consider breathing, pressure management, abdominal wall tension, pelvic floor coordination, pain, symptoms, and function.
For many patients, diastasis recti improves naturally postpartum. For others, individualized rehabilitation may help restore confidence, strength, and trunk control. Co-management with pelvic floor physiotherapy may be helpful when there are pelvic floor symptoms, urinary leakage, pelvic heaviness, pain, or more complex postpartum concerns.
Chiropractic Support Into the Postpartum Period
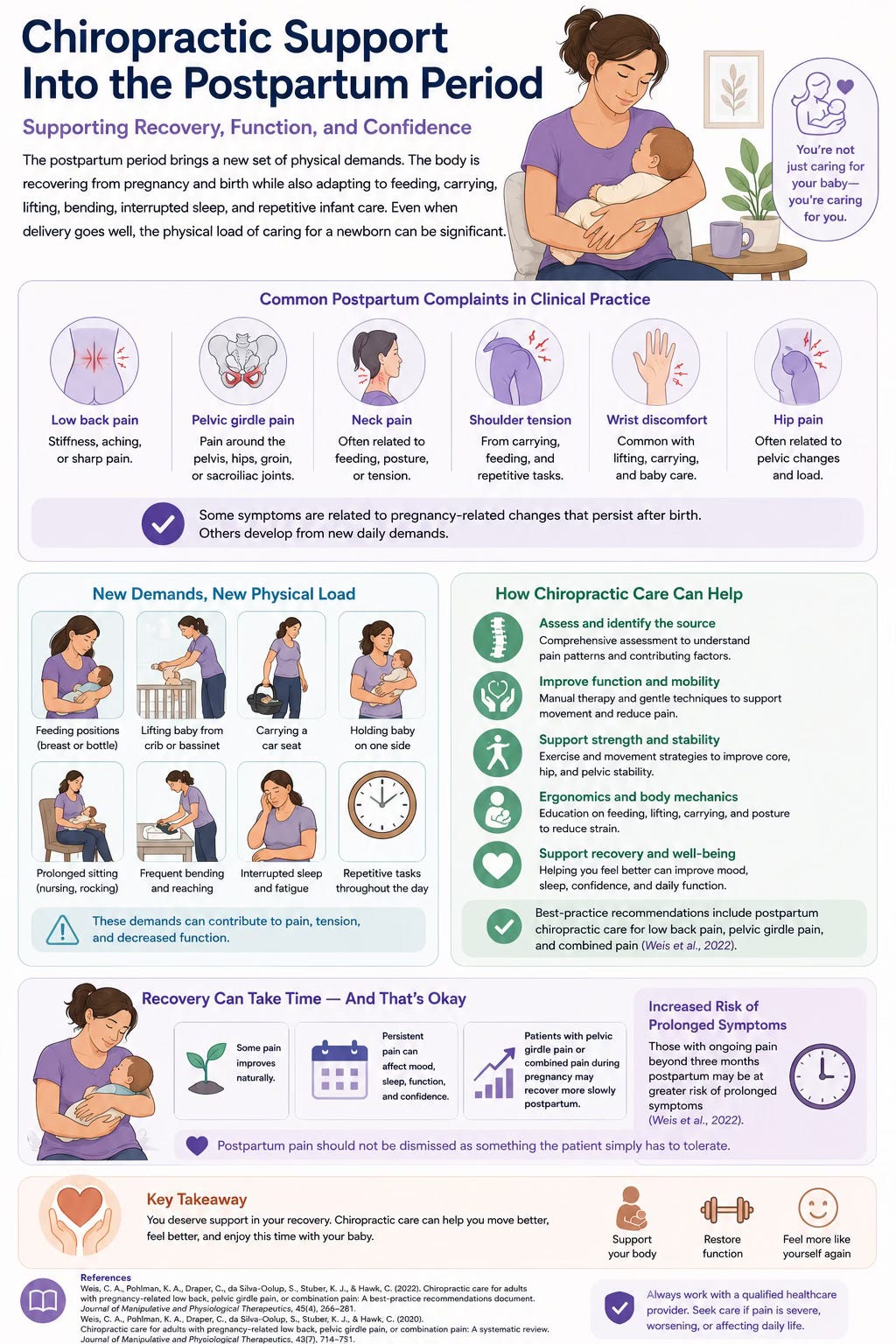
The postpartum period brings a new set of physical demands. The body is recovering from pregnancy and birth while also adapting to feeding, carrying, lifting, bending, interrupted sleep, and repetitive infant care. Even when delivery goes well, the physical load of caring for a newborn can be significant.
Postpartum back pain, pelvic girdle pain, neck pain, shoulder tension, wrist discomfort, and hip pain are common complaints in clinical practice. Some symptoms are related to pregnancy-related changes that persist after birth. Others develop from new daily demands such as feeding positions, lifting the baby from a crib, carrying a car seat, holding the baby on one side, or prolonged sitting.
Best-practice recommendations include postpartum chiropractic care for low back pain, pelvic girdle pain, and combined pain, with appropriate assessment and management based on the patient’s presentation (Weis et al., 2022).
Postpartum pain should not be dismissed as something the patient simply has to tolerate. Some pain improves naturally, but persistent pain can affect mood, sleep, function, and confidence. Patients with pelvic girdle pain or combined pain during pregnancy may recover more slowly postpartum, and those with ongoing pain beyond three months may be at greater risk of prolonged symptoms (Weis et al., 2022).
Feeding Posture, Lifting, and Infant Care Ergonomics
After birth, many parents spend hours feeding, holding, rocking, carrying, and soothing their baby. These tasks are meaningful and necessary, but they can place repetitive stress on the neck, shoulders, upper back, low back, wrists, and hips.
Feeding posture is a common issue. Whether breast/chest feeding or bottle feeding, parents may sit with the head forward, shoulders rounded, upper back flexed, and arms unsupported for long periods. Over time, this can contribute to neck pain, upper back tension, headaches, shoulder discomfort, or wrist strain.
Chiropractors can help patients adjust feeding posture by encouraging better support. This may include bringing the baby toward the parent rather than the parent collapsing toward the baby, using pillows to support the arms, changing sides, keeping the feet supported, and taking brief posture breaks when possible.
Lifting and carrying strategies are also important. Parents may benefit from learning how to hinge at the hips, keep loads close, avoid twisting while lifting, alternate carrying sides, and reduce repetitive strain when lifting from cribs, car seats, or strollers.
Small changes can make a meaningful difference when repeated dozens of times per day.
A Practical Example: Why Individualized Care Matters
Consider two pregnant patients with low back and pelvic discomfort.
The first patient is 24 weeks pregnant and has mild low back stiffness after sitting at work. Her pain improves with walking and gentle movement. She has no red flags and her pregnancy is uncomplicated. Her care plan may focus on education, workstation modifications, gentle mobility, walking breaks, low-force manual therapy if appropriate, and home exercises for hip and trunk support.
The second patient is 32 weeks pregnant and has sharp pelvic pain with rolling in bed, stairs, and standing on one leg. She feels unstable and avoids walking because of pain. Her assessment may suggest pelvic girdle pain rather than simple low back pain. Her plan may involve activity modification, pelvic support strategies, careful exercise selection, avoiding aggravating positions, manual therapy adapted to comfort, and possible co-management with pelvic floor physiotherapy or her prenatal provider if needed.
Both patients are pregnant. Both have back or pelvic pain. But their care plans should not be identical.
That is the value of assessment.
The Bottom Line
Pregnancy and postpartum recovery place new demands on the spine, pelvis, muscles, joints, abdominal wall, pelvic floor, and nervous system. Low back pain, pelvic girdle pain, and combined pain are common, but they should not be dismissed as something patients simply have to endure.
Chiropractic care during pregnancy and postpartum may help by providing education, assessment, manual therapy when appropriate, exercise guidance, ergonomic strategies, support devices when appropriate, and support for daily function. Best-practice recommendations emphasize informed consent, red flag screening, individualized care, modified treatment techniques, interprofessional collaboration, and active rehabilitation (Weis et al., 2022).
Physical activity is also a key part of pregnancy health. The 2019 Canadian Guideline for Physical Activity Throughout Pregnancy recommends at least 150 minutes of moderate-intensity physical activity per week for pregnant individuals without contraindications, accumulated over at least three days per week, with a combination of aerobic and resistance training encouraged (Mottola et al., 2018).
The goal is not only pain relief. The goal is to help patients move with more confidence, stay active safely, manage physical demands, and transition into postpartum recovery with support.
At The Muscle and Joint Clinic, we provide pregnancy and postpartum care that is individualized to the patient’s symptoms, stage of pregnancy or recovery, health history, comfort level, and goals. Whether someone is dealing with low back pain, pelvic girdle pain, hip discomfort, posture changes, feeding-related neck pain, or return-to-exercise questions, an appropriate assessment can help determine the safest and most effective plan.
Pregnancy changes the body. Care should change with it.
Disclaimer
This article is for general educational purposes only and is not intended to provide medical advice, diagnosis, or treatment. Chiropractic care and exercise during pregnancy and postpartum should be individualized based on health history, pregnancy stage, symptoms, risk factors, contraindications, and guidance from prenatal or postpartum healthcare providers. If you have vaginal bleeding, severe abdominal or pelvic pain, signs of preeclampsia, chest pain, shortness of breath, dizziness, trauma, high blood pressure, loss of fluid, painful contractions, or any pregnancy-related complication, seek medical care immediately. Always speak with a qualified healthcare provider before starting or changing an exercise or treatment plan during pregnancy or postpartum.
References
Canadian Chiropractic Association. (2026, April 29). Five reasons to see a chiropractor during pregnancy. Canadian Chiropractic Association.
George, J. W., Skaggs, C. D., Thompson, P. A., Nelson, D. M., Gavard, J. A., & Gross, G. A. (2013). A randomized controlled trial comparing a multimodal intervention and standard obstetrics care for low back and pelvic pain in pregnancy. American Journal of Obstetrics and Gynecology, 208(4), 295.e1–295.e7.
Mottola, M. F., Davenport, M. H., Ruchat, S.-M., Davies, G. A., Poitras, V. J., Gray, C. E., Jaramillo Garcia, A., Barrowman, N., Adamo, K. B., Duggan, M., Barakat, R., Chilibeck, P., Fleming, K., Forte, M., Korolnek, J., Nagpal, T., Slater, L. G., Stirling, D., & Zehr, L. (2018). 2019 Canadian guideline for physical activity throughout pregnancy. British Journal of Sports Medicine, 52(21), 1339–1346. https://doi.org/10.1136/bjsports-2018-100056
Vleeming, A., Albert, H. B., Ostgaard, H. C., Sturesson, B., & Stuge, B. (2008). European guidelines for the diagnosis and treatment of pelvic girdle pain. European Spine Journal, 17(6), 794–819.
Weis, C. A., Pohlman, K. A., Barrett, J., Clinton, S., da Silva-Oolup, S., Draper, C., Lee, J., Kumar, R., O’Beirne, M., Stuber, K., & Hawk, C. (2022). Best-practice recommendations for chiropractic care for pregnant and postpartum patients: Results of a consensus process. Journal of Manipulative and Physiological Therapeutics, 45(7), 469–489. https://doi.org/10.1016/j.jmpt.2021.03.002
Weis, C. A., Pohlman, K. A., Draper, C., da Silva-Oolup, S., Stuber, K., & Hawk, C. (2020). Chiropractic care for adults with pregnancy-related low back, pelvic girdle pain, or combination pain: A systematic review. Journal of Manipulative and Physiological Therapeutics, 43(7), 714–731. https://doi.org/10.1016/j.jmpt.2020.05.005