
Frozen Shoulder
What It Is, Why It Happens, and How Treatment Can Help


Frozen shoulder, also called adhesive capsulitis, is a condition that causes shoulder pain, stiffness, and a major loss of movement. It often starts gradually, gets worse over time, and can make simple things like reaching overhead, putting on a shirt, fastening a bra, washing hair, or reaching behind your back surprisingly difficult. Although it is often described as something that will “eventually go away,” newer evidence suggests that many people can have symptoms for a long time, and some do not fully recover without proper treatment (Achilova et al., 2026; Challoumas et al., 2020).
What exactly is frozen shoulder?
Frozen shoulder is not just ordinary shoulder soreness. It involves irritation and thickening of the shoulder capsule, the connective tissue surrounding the shoulder joint, which can lead to pain and a marked loss of motion, especially passive motion, meaning even someone else moving your arm feels restricted. Diagnosis is usually based on the history and physical exam, particularly when there is a global restriction of shoulder movement without another obvious cause on imaging. X-rays are often normal, and imaging is usually used more to rule out other problems than to “prove” frozen shoulder itself (Achilova et al., 2026; Challoumas et al., 2020).
Common symptoms of frozen shoulder
Most people notice a combination of:
a deep, aching shoulder pain
worsening stiffness
difficulty reaching overhead or behind the back
trouble sleeping on the affected side
pain with everyday tasks like dressing, grooming, lifting, or putting on a coat
Frozen shoulder is often described as moving through overlapping phases: a painful or “freezing” stage, a stiff or “frozen” stage, and a gradual recovery or “thawing” stage. That said, recovery does not always happen quickly. Some studies suggest symptoms may last many months, and in some people the problem can linger far longer than expected (Challoumas et al., 2020; Achilova et al., 2026).

Who gets frozen shoulder?
Frozen shoulder is common in middle-aged adults and is seen more often in people with diabetes and some other metabolic or systemic conditions. It can also develop after a period of shoulder pain, reduced use, injury, or surgery, although many cases appear without one obvious trigger (Achilova et al., 2026).
How is frozen shoulder treated?
Treatment depends on the stage of the condition, symptom severity, and the individual patient. In general, most cases are treated without surgery at first. The strongest evidence supports a combination of guided exercise/physical therapy, activity modification, and in selected cases intra-articular corticosteroid injection, especially earlier in the course when pain is a dominant problem (Achilova et al., 2026; Challoumas et al., 2020).
A large systematic review and meta-analysis found that intra-articular corticosteroid injection was associated with meaningful short-term improvements, and the addition of physiotherapy or a home exercise program may provide added benefit. The same review found that treatment results vary depending on timing and the intervention used, which is why individualized care matters (Challoumas et al., 2020).
Hydrodilatation, also called capsular distension, may help some patients, particularly for pain relief, and surgical options such as manipulation under anesthesia or arthroscopic capsular release are typically reserved for more stubborn cases after months of failed conservative care (Challoumas et al., 2020; Mullen et al., 2025).
Where do shockwave and laser therapy fit in?
This is where many patients have questions.
Shockwave therapy
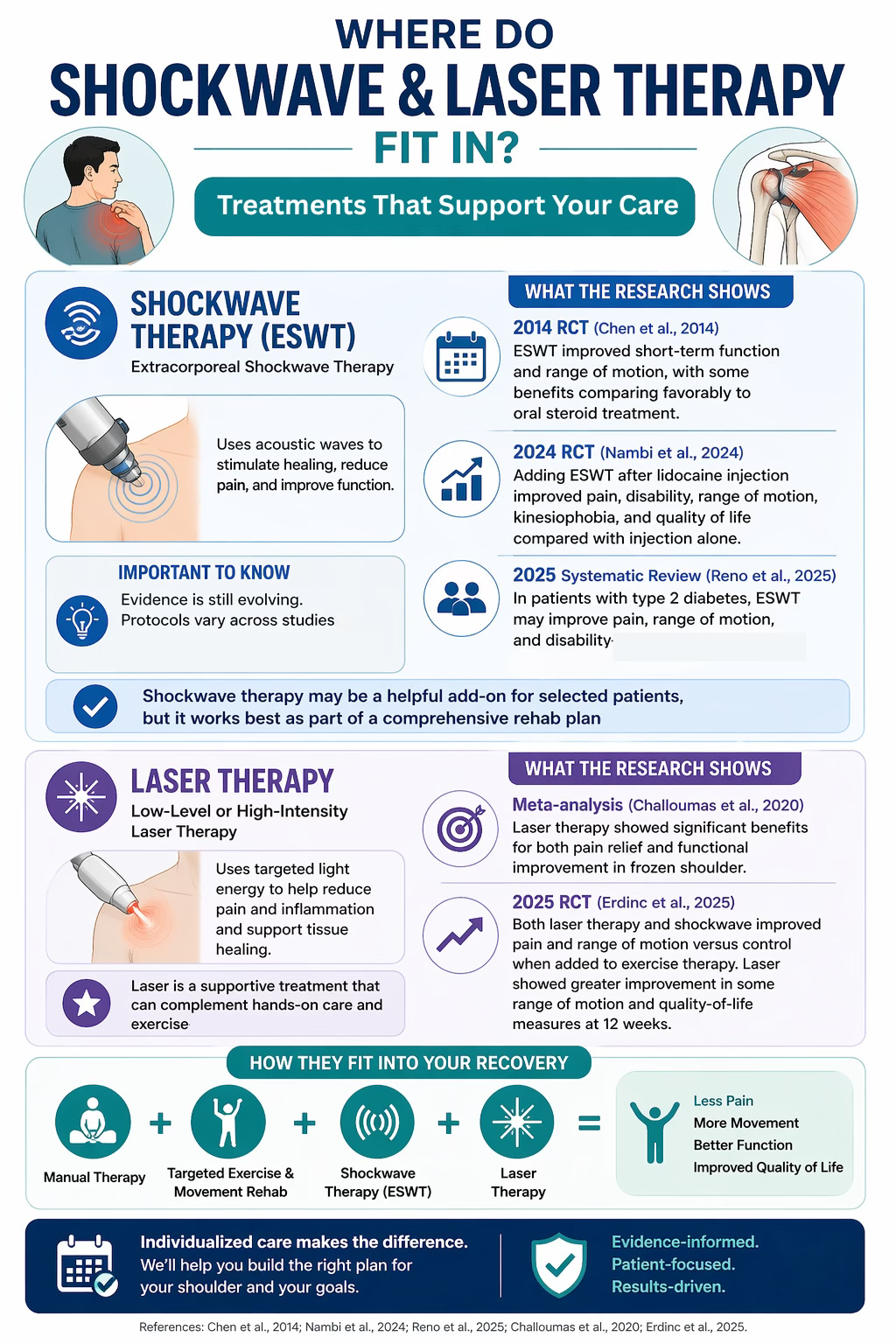
Extracorporeal shockwave therapy (ESWT) has been studied as a useful adjunct in conservative care. A 2014 randomized controlled trial found that ESWT improved short-term function and range of motion, with some benefits comparing favorably to oral steroid treatment in the short term (Chen et al., 2014). A more recent randomized trial reported that adding ESWT after lidocaine injection improved pain, disability, range of motion, kinesiophobia, and quality of life compared with injection alone (Nambi et al., 2024). A 2025 systematic review in patients with type 2 diabetes also found that ESWT may improve pain, range of motion, and disability, though the authors noted that better-quality studies are still needed (Reno et al., 2025).
That said, the evidence is still evolving. Protocols vary across studies, and not every review concludes the same thing. So the best way to think about shockwave is this: it may be a helpful add-on for selected patients, but it should be used as part of a broader rehab plan rather than as a magic fix on its own (Reno et al., 2025).
Laser therapy
Laser therapy is another modality that may be used as an adjunct to help manage pain and support function. In the frozen shoulder literature, both low-level and higher-intensity laser approaches have been studied. The 2020 meta-analysis by Challoumas and colleagues included laser among the nonsurgical treatments studied for frozen shoulder, and more recent comparative research suggests that both ESWT and low-intensity laser therapy, when added to exercise therapy, can improve pain and range of motion. In one 2025 randomized trial, both helped, while the laser group showed greater improvement in some range-of-motion and quality-of-life measures at 12 weeks (Challoumas et al., 2020; Erdinc et al., 2025).
Like shockwave, laser should be viewed as a supportive treatment, not a standalone cure. The foundation of care is still the bigger plan: reducing irritability, improving mobility, restoring function, and helping the shoulder tolerate movement again (Achilova et al., 2026).
How our clinic can help
At The Muscle & Joint Clinic, treatment for frozen shoulder focuses on helping patients move better, reduce pain, and gradually regain function with a plan that fits the stage of the condition.
Depending on the patient, care may include:
a detailed assessment to help determine whether the shoulder is behaving like frozen shoulder or another condition
guided mobility and range-of-motion work
manual therapy where appropriate
progressive rehab exercises based on irritability and tolerance
advice on activity modification and pacing
shockwave therapy as an adjunct for selected cases
laser therapy as an adjunct to support pain relief and function
coordination with your physician if medical imaging, injection, or specialist referral is appropriate
Our goal is not to promise an instant fix. Frozen shoulder can be stubborn. The real goal is to help calm the painful phase, improve movement safely, and build a steady path back to daily activities. For some patients, adjunctive options like shockwave or laser therapy may be useful as part of that broader plan, especially when combined with hands-on care and exercise rather than used in isolation. This approach is consistent with the broader literature showing that multimodal, individualized treatment tends to make the most sense for frozen shoulder management (Achilova et al., 2026; Challoumas et al., 2020).
When should you get assessed?
It is worth getting your shoulder checked if:
pain and stiffness have been building over weeks or months
you cannot reach overhead or behind your back the way you used to
your sleep is being disrupted
stretching on your own is not helping
your shoulder feels like it is getting more restricted, not less
The earlier a proper diagnosis is made, the easier it is to guide treatment appropriately and avoid wasting time on the wrong approach (Achilova et al., 2026).

Final thoughts
Frozen shoulder is more than “just a stiff shoulder.” It can be frustrating, painful, and slow to improve. The good news is that many people do respond well to conservative treatment, especially when care is matched to the stage of the condition and the person’s needs. Exercise-based rehab remains central, injections may help in selected cases, and treatments like shockwave therapy and laser therapy may offer additional support for some patients as part of a complete plan (Achilova et al., 2026; Challoumas et al., 2020; Chen et al., 2014; Nambi et al., 2024; Reno et al., 2025).
If you have been dealing with persistent shoulder pain and stiffness, a proper assessment can help clarify what is going on and what treatment options make the most sense for you.
References
Achilova, F., Daher, M., Nassar, J. E., Daniels, A. H., & Abboud, J. A. (2026). Frozen shoulder: Diagnosis and treatment of adhesive capsulitis. The American Journal of Medicine, 139(5), 598–605. https://doi.org/10.1016/j.amjmed.2026.01.021
Challoumas, D., Biddle, M., McLean, M., & Millar, N. L. (2020). Comparison of treatments for frozen shoulder: A systematic review and meta-analysis. JAMA Network Open, 3(12), e2029581. https://doi.org/10.1001/jamanetworkopen.2020.29581
Chen, C.-Y., Hu, C.-C., Weng, P.-W., Huang, Y.-M., Chiang, C.-J., Chen, C.-H., Tsuang, Y.-H., Yang, R.-S., Sun, J.-S., & Cheng, C.-K. (2014). Extracorporeal shockwave therapy improves short-term functional outcomes of shoulder adhesive capsulitis. Journal of Shoulder and Elbow Surgery, 23(12), 1843–1851. https://doi.org/10.1016/j.jse.2014.08.010
Erdinc, F., Tuncay, F., Ceylan, İ., Karacay, B. C., & Kapan, N. (2025). Effects of low-intensity extracorporeal shockwave therapy and low-intensity laser therapy on shoulder adhesive capsulitis. American Journal of Physical Medicine & Rehabilitation. Advance online publication.
(Note: verify final volume, issue, and page numbers before publication if you want a fully finalized APA entry.)
Mullen, J. P., Hauer, T. M., Lau, E. N., & Lin, A. (2025). Adhesive capsulitis of the shoulder. Arthroscopy: The Journal of Arthroscopic & Related Surgery.
(Note: verify final volume, issue, and page numbers before publication if you want a fully finalized APA entry.)
Nambi, G., Alghadier, M., Eltayeb, M. M., et al. (2024). Additional effect of extracorporeal shockwave therapy with lidocaine injection on clinical and MRI findings in frozen shoulder: A prospective, randomized, double-blinded, placebo-controlled trial. Pain and Therapy.
(Note: verify final volume, issue, and page numbers before publication if you want a fully finalized APA entry.)
Reno, C., Swinton, P. A., & Alexander, L. (2025). Extracorporeal shock wave therapy for chronic adhesive capsulitis in type 2 diabetics: A systematic review with meta-analysis. Physical Therapy, 105(7), pzaf074. https://doi.org/10.1093/ptj/pzaf074