
How Chiropractic Care Helps Cervicogenic Headaches
What the Evidence Actually Shows


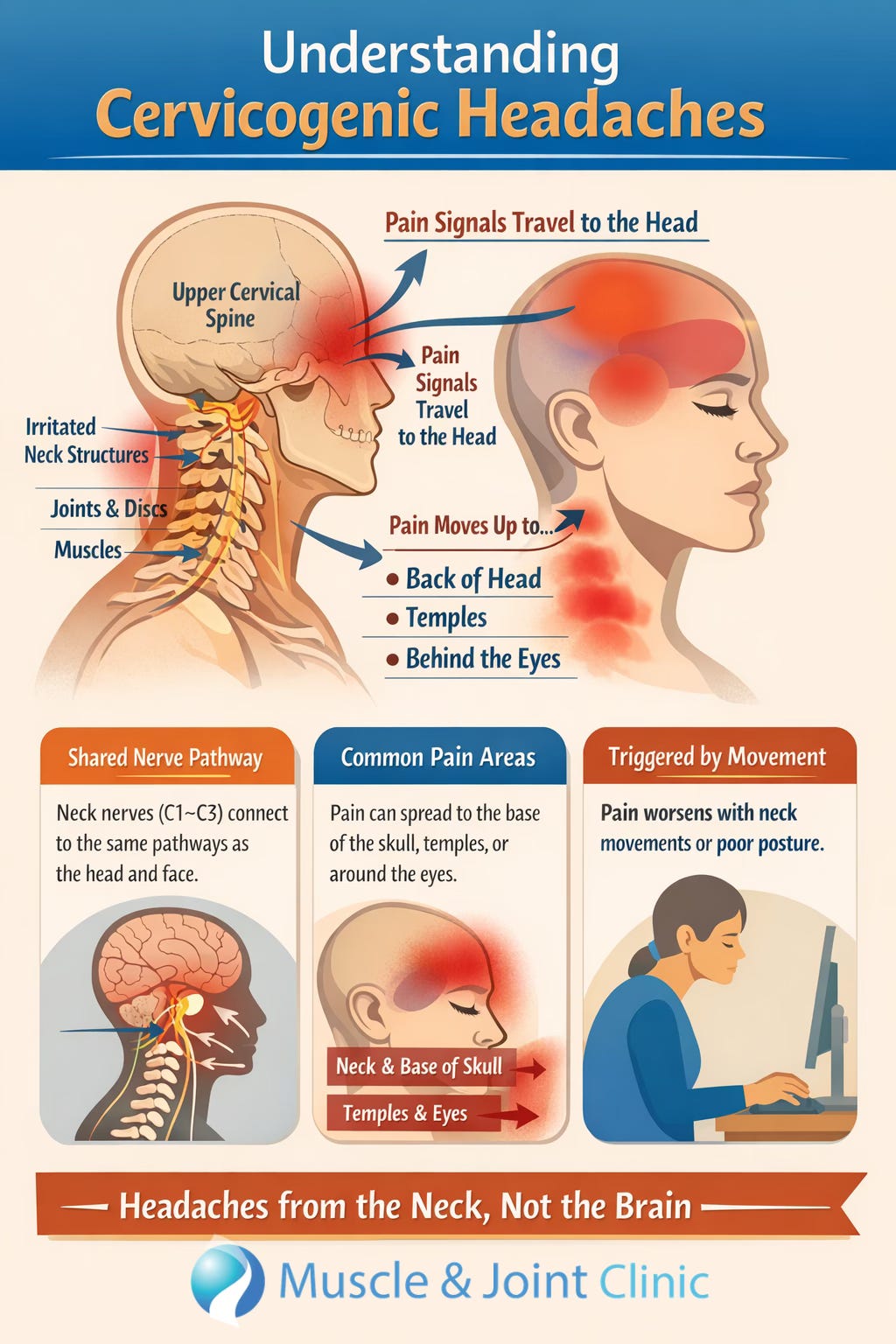
Cervicogenic headaches are a type of headache that come from the neck, not the brain. In this condition, structures in the upper neck, such as the joints, discs, and surrounding muscles, send pain signals up into the head. This happens because the nerves from the upper cervical spine (especially C1–C3) connect with the same pathways that carry sensation from the face and head. When something in the neck becomes irritated, stiff, or inflamed, the brain can interpret that signal as a headache. This is why people with cervicogenic headaches often feel pain that starts in the neck and moves up into the back of the head, temples, or even behind the eyes, and why the pain tends to get worse with certain neck movements or prolonged postures.
From a mechanical perspective, the upper neck plays a critical role in both movement and stability. The joints between the first few vertebrae are responsible for a large portion of head rotation and fine control. Surrounding these joints are small but important muscles that help guide movement and maintain proper alignment. When these joints become restricted or the muscles become tight or overworked, often due to posture, repetitive strain, or previous injury, the normal signals from the neck to the brain can become disrupted. This can increase sensitivity in the nervous system and lead to the development of persistent headaches. Over time, the body may also compensate by changing how it moves, which can further reinforce the problem.
Recent research has helped clarify the most effective ways to treat this type of headache. A large 2026 study that analyzed over 40 clinical trials and nearly 2,000 patients found that treatments that combine multiple approaches, rather than relying on a single therapy, lead to the best results. These “multimodal” treatments typically include a combination of hands-on care (manual therapy), muscle-based treatments (like dry needling or soft tissue work), and guided exercise programs. Together, these approaches were shown to significantly reduce headache intensity, decrease how often headaches occur, and improve overall function and quality of life. In contrast, treatments used on their own, such as massage alone or medications like pregabalin or botulinum toxin, were found to be less effective for long-term improvement (Koonalinthip et al., 2026).

The reason this combined approach works so well comes down to how the body functions as a system. Manual therapy helps restore movement in the joints of the neck, which reduces irritation and improves how the joints communicate with the nervous system. Muscle-based treatments help release tight or overactive muscles and improve blood flow, which can reduce pain and sensitivity. Exercise then reinforces these changes by strengthening the muscles, improving coordination, and helping the body maintain better posture and movement patterns over time. Instead of just temporarily relieving symptoms, this approach addresses both the cause of the problem and the factors that keep it going.
Another important point is that not all treatments target the source of cervicogenic headaches equally. Because the problem originates in the upper neck, treatments that directly address this area tend to be more effective than those that focus elsewhere. While general massage or medications may provide temporary relief, they do not correct the underlying joint or movement dysfunction. This is why many patients find that their headaches return once these treatments are stopped. In contrast, care that focuses on restoring normal movement and function in the neck can produce longer-lasting results because it addresses the root cause of the pain.
Overall, the current evidence supports a clear and practical message for patients: cervicogenic headaches are best treated by focusing on the neck itself and by using a combination of therapies that work together. By improving joint mobility, reducing muscle tension, and restoring healthy movement patterns, it is possible to significantly reduce both the frequency and severity of headaches and improve overall quality of life.
References
Koonalinthip, N., Koonalintip, P., & Stonsaovapak, C. (2026). The comparative efficacy of treatments for cervicogenic headache: A systematic review and network meta-analysis of randomized controlled trials. European Journal of Pain, 30(2), e70219. https://doi.org/10.1002/ejp.70219
Nambi, G., Alghadier, M., Eltayeb, M. M., Aldhafian, O. R., Saleh, A. K., Alsanousi, N., Albarakati, A. J. A., Omar, M. A., Ibrahim, M. N. A., Attallah, A. A., Ismail, M. A., & Elfeshawy, M. (2024). Comparative effectiveness of cervical vs thoracic spinal-thrust manipulation for care of cervicogenic headache: A randomized controlled trial. PLOS One, 19(3), e0300737. https://doi.org/10.1371/journal.pone.0300737