
Lumbar Spinal Stenosis: Why It Happens, Why Walking Becomes Difficult, and How Chiropractic Care May Help


Lumbar spinal stenosis is one of the most common spine conditions affecting older adults. It is also one of the most common reasons people over the age of 60 seek care for low back pain, leg pain, difficulty walking, and reduced mobility. For many patients, the symptoms can be confusing because they do not always behave like a typical muscle strain or disc injury. A person may feel relatively comfortable while sitting, but then develop pain, heaviness, numbness, tingling, or weakness in the legs after standing or walking for a period of time. The symptoms may force them to stop, sit down, lean forward, or rest before they can continue.
At The Muscle and Joint Clinic, we often see patients who describe this classic pattern. They may say they can walk farther when leaning on a shopping cart, that standing in one place is harder than sitting, or that walking downhill bothers them more than walking uphill. Some people feel pressure in the low back. Others feel symptoms mainly in the buttocks, thighs, calves, or feet. Some patients do not have much back pain at all, but they notice their legs become tired, heavy, or uncomfortable when they walk.
Lumbar spinal stenosis can be frustrating because it often affects independence. It can make grocery shopping harder. It can limit travelling, walking for exercise, standing in lines, gardening, household chores, and playing with grandchildren. Many people slowly reduce their activity because they are worried symptoms will flare. Over time, this reduction in activity can lead to stiffness, weakness, loss of endurance, balance changes, and reduced confidence.

The good news is that lumbar spinal stenosis does not always mean a person is destined to decline or needs surgery right away. Research has shown that many patients can improve with nonsurgical care. A 2019 randomized clinical trial published in JAMA Network Open compared three nonsurgical treatment approaches for lumbar spinal stenosis: medical care, group exercise, and manual therapy combined with individualized exercise. All three groups improved over time, especially in walking capacity. However, the group that received manual therapy plus individualized exercise had better short-term improvement in symptoms, function, and walking ability at two months compared with the other groups.
This finding is important for patients because it supports what many clinicians see in practice. Lumbar spinal stenosis is often related to structural age-related changes in the spine, but symptoms are influenced by much more than imaging alone. Mobility, strength, hip function, nerve sensitivity, walking tolerance, posture, balance, and confidence all matter. A thoughtful conservative care plan can often help patients move better, walk farther, and manage symptoms more effectively.
What Is Lumbar Spinal Stenosis?
The lumbar spine is the lower part of the spine. It is made up of five vertebrae, which are the bones of the spine. Between these bones are discs, which act as cushions and help with movement. At the back of the spine are small joints called facet joints. Ligaments help support the spine, and muscles around the back, pelvis, hips, and abdomen help provide stability and movement control.
Inside the spine is the spinal canal. This is the space where the spinal cord and nerve structures travel. In the lower back, the spinal cord has usually already ended, and the canal contains nerve roots that travel into the pelvis and legs. These nerves help control sensation, muscle function, reflexes, and movement.
Lumbar spinal stenosis means there is narrowing of the space available for these nerve structures. This narrowing can occur in the central spinal canal, in the side channels where the nerves travel, or in the openings where nerves exit the spine. When the available space becomes reduced, the nerves may become irritated or compressed, especially during positions or activities that further reduce that space.
In many cases, lumbar spinal stenosis develops gradually over time. It is commonly associated with age-related degenerative changes. These changes may include disc degeneration, disc bulging, arthritis of the facet joints, thickening of spinal ligaments, bone spur formation, and sometimes a condition called spondylolisthesis, where one vertebra shifts slightly forward relative to another. These changes can narrow the spaces around the nerves.
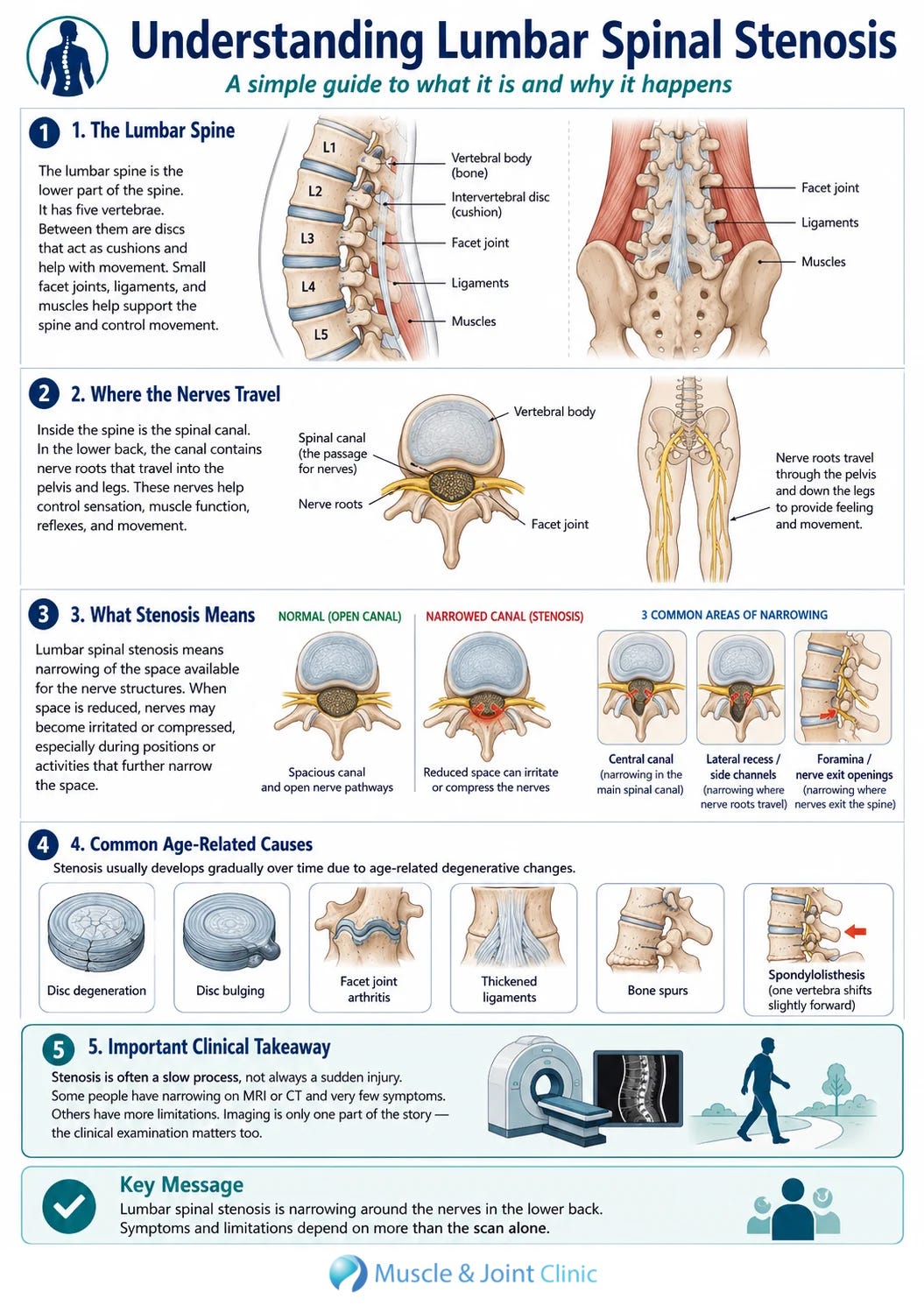
It is important to understand that stenosis is not always a sudden injury. For many people, it is a slow process that develops over years. A person may have narrowing on an MRI or CT scan long before they develop symptoms. Some people have significant narrowing on imaging and only mild symptoms, while others may have moderate narrowing and more significant limitations. This is why the clinical examination matters. The scan is only one part of the story.
Why Imaging Does Not Tell the Whole Story
Many patients become concerned when they hear words like degeneration, arthritis, narrowing, compression, or stenosis on an imaging report. These terms can sound alarming. However, imaging findings must always be interpreted in context. Degenerative changes are very common as people age, and not all degenerative changes cause pain.
A person’s symptoms depend on several factors. These include the degree of narrowing, the location of the narrowing, how sensitive the nerves are, the person’s walking tolerance, posture, strength, flexibility, inflammation level, activity habits, general health, and confidence with movement. Two people can have similar MRI findings but very different symptoms and function.
This is why a diagnosis of lumbar spinal stenosis should not be based on imaging alone. A good assessment looks at the patient’s history, symptom pattern, walking ability, range of motion, neurological function, hip mobility, strength, balance, and response to different positions. In lumbar spinal stenosis, the story the patient tells is often just as important as the scan itself.
One of the most important clinical clues is how symptoms respond to posture. Many people with lumbar spinal stenosis feel worse when standing tall or extending the lower back. They may feel better when sitting, bending forward, or leaning on something. This happens because lumbar extension can reduce the space available in the spinal canal, while lumbar flexion can slightly open that space. This does not mean bending forward fixes the stenosis, but it can temporarily reduce irritation of the nerve structures.
The Classic Symptom Pattern
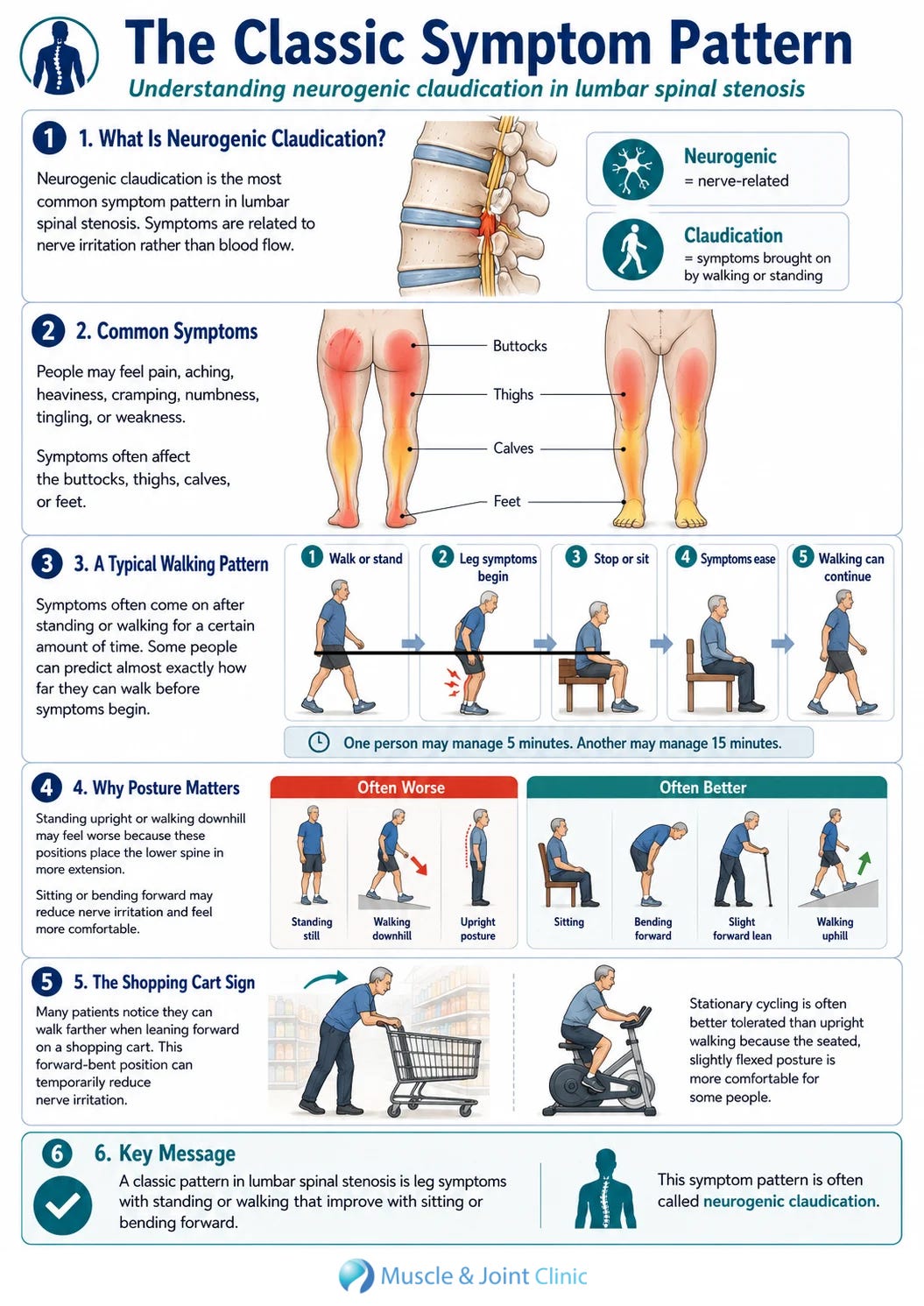
The most common symptom pattern associated with lumbar spinal stenosis is called neurogenic claudication. The word claudication refers to symptoms that come on with walking or standing. Neurogenic means the symptoms are related to nerve irritation rather than blood flow. In lumbar spinal stenosis, neurogenic claudication often causes pain, aching, heaviness, cramping, numbness, tingling, or weakness in the buttocks, thighs, calves, or feet.
Patients may describe needing to stop after walking a certain distance. Some can predict almost exactly how far they can walk before symptoms begin. For example, one person may be able to walk for five minutes before leg heaviness starts, while another may manage fifteen minutes before needing to sit. After sitting or bending forward, the symptoms may ease, allowing the person to continue.
Standing in one place can sometimes be worse than walking. This can happen because standing upright places the lumbar spine in a more extended position. Walking may also become difficult, but some people tolerate slow walking better than prolonged standing. Others find that walking uphill is easier than walking downhill because uphill walking naturally encourages a slight forward lean, while downhill walking often places the spine into more extension.
The shopping cart sign is another common clue. Patients may notice that they can walk farther in a grocery store when leaning forward on a cart. The forward-bent position can temporarily reduce nerve irritation, allowing them to tolerate more walking. This is one reason stationary cycling is often better tolerated than upright walking for some patients with stenosis. The seated, slightly flexed posture can be more comfortable.
How Lumbar Spinal Stenosis Affects Daily Life
Lumbar spinal stenosis can have a major effect on quality of life because walking is central to independence. When walking becomes limited, many daily activities become harder. Patients may avoid malls, airports, long parking lots, community events, family outings, or travel. They may become nervous about going places where they are unsure if seating will be available. Some people begin planning their day around where they can sit and rest.
This can lead to a cycle of reduced activity. A patient walks less because walking triggers symptoms. Because they walk less, their leg strength and endurance decline. As endurance declines, walking becomes harder. As walking becomes harder, the patient becomes less confident and avoids more activity. Over time, this can contribute to deconditioning, stiffness, balance issues, and increased risk of falls.
This cycle is important because conservative care is not only about pain relief. It is also about maintaining function. The goal is to help the patient stay active, preserve independence, and gradually improve tolerance for meaningful activities. Even if the structural narrowing remains present, the patient may still become stronger, more mobile, more confident, and more capable.
What the 2019 JAMA Network Open Study Looked At
The 2019 randomized clinical trial by Schneider and colleagues studied 259 adults with lumbar spinal stenosis. The average age of participants was approximately 72 years. To be included, patients had to have imaging evidence of lumbar spinal stenosis on MRI or CT, along with clinical symptoms consistent with the condition. These symptoms included leg symptoms that worsened with walking and improved with sitting, symptoms worsened by lumbar extension and relieved by flexion, or leg pain relieved by leaning forward on a shopping cart.
The participants were randomly assigned to one of three treatment groups. One group received medical care from a physical medicine physician. This care included medications such as anti-inflammatory medication, acetaminophen, nerve-related medications, or other non-opioid medications. The physician also had the option of referring patients for epidural steroid injections when appropriate.
A second group participated in supervised group exercise classes at community centers. These classes were designed for older adults and were supervised by fitness instructors. The goal was to provide general exercise in a community setting.
The third group received manual therapy combined with individualized exercise. This care was provided by chiropractors and physical therapists. The treatment included a warm-up on a stationary bike, manual therapy procedures such as lumbar distraction mobilization, hip joint mobilization, lumbar and sacroiliac mobilization, neural mobilization, and individualized instruction in stabilization exercises and home stretching.
All treatments were delivered over six weeks. The researchers then measured outcomes at two months and six months. They looked at self-reported symptoms and function using the Swiss Spinal Stenosis questionnaire, walking capacity using a self-paced walking test, and physical activity using an activity monitor.
What the Study Found
The study found that all three groups improved over time. This alone is an encouraging finding. Lumbar spinal stenosis is often considered a chronic degenerative condition, but the study showed that patients can improve with nonsurgical care. In particular, walking capacity improved across all three groups and these improvements were still present at six months.
At the two-month follow-up, the manual therapy and individualized exercise group had greater improvement in symptoms and physical function compared with medical care and group exercise. This group also had a higher proportion of patients who achieved at least a 30 percent improvement in walking capacity. At two months, 65.3 percent of patients in the manual therapy and individualized exercise group achieved at least 30 percent improvement in walking capacity. This compared with 48.7 percent in the medical care group and 46.2 percent in the group exercise group.
The manual therapy and individualized exercise group also had a higher proportion of patients with at least 30 percent improvement in symptoms and function at two months. This suggests that a more individualized, hands-on, active rehabilitation approach may provide stronger short-term benefits for some patients with lumbar spinal stenosis.
By six months, however, there were no significant differences between the groups. This means that while manual therapy and individualized exercise appeared to provide better short-term outcomes, the longer-term outcomes were similar among the three approaches. This does not make the short-term improvement unimportant. For a patient who is struggling to walk, sleep, shop, travel, or function, meaningful improvement over the first several weeks can be very valuable. It may also help the patient become more active, more confident, and more engaged in their recovery.
Why Manual Therapy and Individualized Exercise May Help
Manual therapy and individualized exercise may help patients with lumbar spinal stenosis for several reasons. The goal is not to “reverse” arthritis or permanently enlarge the spinal canal. Degenerative changes in the spine cannot simply be adjusted away. Instead, conservative care focuses on improving the factors that can influence symptoms and function.
Many patients with lumbar spinal stenosis have stiffness in the lumbar spine, hips, pelvis, and surrounding soft tissues. They may also have weakness in the gluteal muscles, reduced core endurance, poor balance, tight hip flexors, limited walking tolerance, and sensitivity of the nerve tissues. These factors can affect posture, movement, and loading through the lower back.
Manual therapy may help reduce stiffness, improve joint movement, decrease muscle guarding, and make it easier for patients to exercise. Hip mobilization may be especially relevant because hip stiffness can change walking mechanics and increase demand on the lower back. Lumbar mobilization and gentle distraction-based techniques may help some patients tolerate movement better. Neural mobilization may be used when nerve sensitivity is contributing to leg symptoms, although it must be applied carefully and matched to the patient’s tolerance.
Individualized exercise is equally important. Exercise helps improve strength, endurance, balance, mobility, and confidence. A patient with spinal stenosis may need a specific program that respects their symptom pattern. For example, some patients tolerate flexion-biased exercises better than extension-based exercises. Others may need to start with seated or supported exercises before progressing to standing exercises. Some may benefit from stationary cycling before walking progression. The program should be based on the patient, not a generic handout.
Why General Exercise Alone May Not Be Enough for Some Patients
General exercise is still valuable. Movement is important for older adults, and group exercise can improve confidence, social engagement, cardiovascular health, and general conditioning. For some patients with mild symptoms, a general exercise class may be enough to help them stay active.
However, lumbar spinal stenosis can vary significantly from person to person. One patient may have mostly back stiffness. Another may have severe leg heaviness with walking. Another may have balance concerns, hip arthritis, knee osteoarthritis, diabetes, neuropathy, or other health conditions that affect exercise tolerance. A general class may not address the specific movement restrictions, weakness patterns, nerve sensitivity, or walking limitations that are contributing to the patient’s symptoms.
This is where individualized care can be helpful. A clinician can assess how the patient moves, what triggers symptoms, what relieves symptoms, how far the patient can walk, which exercises are tolerated, and which areas need to be strengthened or mobilized. The treatment plan can then be adjusted based on response. If an exercise flares symptoms, it can be modified. If the patient improves, the program can be progressed. This flexibility is one of the advantages of a personalized approach.
The Importance of Walking Capacity
Walking capacity is one of the most important outcomes for patients with lumbar spinal stenosis. Pain scores matter, but they do not always tell the full story. A patient may still have some discomfort but be able to walk farther, stand longer, and participate in more activities. That can represent a meaningful improvement in quality of life.
In the JAMA Network Open study, walking capacity improved in all three groups. This is clinically important because walking limitation is often the main disability associated with lumbar spinal stenosis. The ability to walk farther can mean being able to shop independently, travel through an airport, attend family events, or return to recreational walking.
At The Muscle and Joint Clinic, walking tolerance is often used as a practical marker of progress. If a patient can only walk for five minutes before symptoms begin, the first goal may be to improve to seven or eight minutes. Then ten minutes. Then fifteen. Progress may be gradual, but these changes can make a major difference in daily life. Treatment should focus not only on reducing pain during a visit, but also on improving what the patient can do outside the clinic.
Why the Hips, Core, and Legs Matter
Although lumbar spinal stenosis is a spinal condition, the hips, pelvis, core, and legs play a major role in how symptoms are experienced. Walking is a full-body activity. If the hips are stiff, the lumbar spine may compensate. If the gluteal muscles are weak, the pelvis and lower back may have to absorb more load. If the core muscles fatigue quickly, posture and movement control may worsen. If the calves, hamstrings, or hip flexors are tight, stride mechanics may change.
Many older adults also have other conditions that interact with spinal stenosis. Knee osteoarthritis, hip osteoarthritis, foot problems, balance issues, neuropathy, and general deconditioning can all influence walking ability. A patient may have stenosis on imaging, but their walking limitation may be partly due to hip weakness, knee pain, poor endurance, or fear of falling. A good assessment should consider all of these factors.
This is why treatment should not focus only on the painful area. Improving hip mobility, lower-body strength, balance, and walking mechanics may reduce stress on the lower back and improve function. In many cases, the most effective plan is not simply a back treatment plan. It is a movement and function plan.
The Role of Chiropractic Care
Chiropractic care for lumbar spinal stenosis should be evidence-informed, patient-specific, and function-focused. The goal is not to claim that chiropractic treatment can cure stenosis or erase degenerative changes. Instead, chiropractic care may help by improving mobility, reducing mechanical sensitivity, addressing contributing movement restrictions, and supporting a progressive exercise plan.
A chiropractor may use gentle spinal mobilization, soft tissue therapy, assisted stretching, hip and pelvic mobilization, flexion-distraction-style approaches, exercise coaching, posture advice, and walking progression strategies. Treatment should be adapted to the patient’s age, irritability level, medical history, imaging findings, neurological status, and goals.
For some patients, hands-on care helps reduce pain enough that they can begin exercising more comfortably. For others, the biggest value comes from education and a structured plan. Patients often need help understanding which movements are safe, how to pace walking, how to avoid overreacting to flare-ups, and how to gradually build tolerance without repeatedly aggravating symptoms.
Chiropractic care may also involve co-management. Some patients benefit from communication between chiropractors, physiotherapists, family physicians, physiatrists, pain specialists, or surgeons. Lumbar spinal stenosis can exist on a spectrum, and the best care depends on severity, progression, neurological findings, and patient preference.
What an Assessment May Include
A proper assessment for suspected lumbar spinal stenosis begins with a detailed history. The clinician will ask where the symptoms are felt, how long they have been present, what brings them on, what relieves them, how far the patient can walk, whether sitting helps, whether leaning forward helps, and whether symptoms are changing over time. The clinician will also ask about numbness, tingling, weakness, balance, falls, bladder or bowel changes, and previous imaging or treatment.
The physical examination may include lumbar range of motion, repeated movement testing, neurological screening, reflexes, sensation, muscle strength, hip mobility, lower-body flexibility, balance, gait, posture, and functional movements such as sit-to-stand or walking tolerance. The goal is to determine whether the symptom pattern is consistent with lumbar spinal stenosis, whether other conditions may be contributing, and whether conservative care is appropriate.
It is also important to distinguish lumbar spinal stenosis from other causes of leg symptoms. Vascular claudication, peripheral neuropathy, hip arthritis, knee arthritis, disc herniation, peripheral nerve entrapment, and other medical conditions can sometimes mimic or overlap with spinal stenosis. For example, vascular claudication is related to blood flow and may also cause leg pain with walking, but the clinical pattern is different. This is why assessment matters.
Conservative Treatment Goals
The first goal of conservative treatment is usually education. Patients often feel more confident when they understand why their symptoms behave the way they do. Knowing that sitting or leaning forward can relieve symptoms because of spinal positioning can help patients make sense of their experience. Education can also reduce fear and help patients stay active in a safer, more strategic way.
The second goal is symptom modulation. This may involve manual therapy, mobility exercises, gentle stretching, supported positions, and activity modification. The purpose is to reduce irritability and make movement feel more tolerable. This phase is especially important for patients who are flared up or nervous about movement.
The third goal is improving mobility and strength. This may include hip mobility work, lumbar mobility exercises, glute strengthening, core stabilization, and lower-body strengthening. The exercises should be selected based on the patient’s presentation. Some patients need very gentle starting points, while others can tolerate more challenging strengthening.
The fourth goal is improving walking tolerance. This is often done through graded exposure. Instead of telling patients to simply walk as much as possible, it may be more effective to use intervals. For example, a patient may walk for a tolerable amount of time, rest briefly, then repeat. Over time, the walking time can gradually increase. This helps build capacity without repeatedly pushing into severe symptoms.
The final goal is long-term self-management. Lumbar spinal stenosis is usually chronic, so patients need strategies they can continue beyond the treatment plan. This may include a home exercise program, walking progression, flare-up plan, posture strategies, and periodic maintenance or reassessment when needed.
Why Flexion Bias Is Often Used
Many patients with lumbar spinal stenosis tolerate flexion-biased movements better than extension-biased movements. Flexion refers to bending forward. Extension refers to bending backward or standing in a more arched position. Because extension can narrow the spinal canal and foraminal spaces, it may aggravate symptoms in some patients. Flexion can temporarily increase space and reduce symptoms.
This is why certain exercises may be more comfortable than others. A stationary bike may feel better than walking on a treadmill. Seated exercises may feel better than standing exercises. Knees-to-chest movements or gentle lumbar flexion may feel relieving. Walking uphill may feel better than walking downhill. Leaning slightly forward while walking may help some patients tolerate more distance.
However, flexion bias does not mean every patient should only bend forward or avoid all extension forever. The spine still needs balanced movement, and treatment should be individualized. Some patients may tolerate certain extension movements well, while others may not. The key is to match exercise selection to the patient’s symptoms and goals.
Flare-Ups and Pacing
Lumbar spinal stenosis symptoms can fluctuate. Patients may have better days and worse days. A flare-up does not always mean the condition is worsening structurally. Symptoms can be influenced by activity level, sleep, stress, prolonged standing, travel, lifting, inflammation, or doing too much too soon.
Pacing is an important part of management. Many patients fall into an all-or-nothing pattern. On a good day, they do too much and flare their symptoms. Then they rest for several days and lose momentum. A better strategy is to establish a baseline level of activity that is tolerable and gradually build from there.
For walking, this may mean stopping before symptoms become severe, resting briefly, and then continuing. Over time, the patient may be able to increase total walking volume. The goal is to build capacity without constantly provoking major flare-ups.
When Surgery May Be Considered
Conservative care can help many patients, but it is not the right answer for every situation. Surgery may be considered when symptoms are severe, progressive, disabling, or not improving despite appropriate nonsurgical care. Surgery may also be considered when there is significant neurological decline, such as worsening weakness, or when quality of life is severely affected.
The decision for surgery should be made carefully and usually involves consultation with a spine specialist. Factors such as imaging findings, neurological status, general health, age, activity goals, and patient preference all matter. Some patients choose surgery because their walking limitation remains severe despite conservative care. Others prefer to continue nonsurgical management if symptoms are stable and function is acceptable.
It is also important to recognize urgent warning signs. New loss of bladder or bowel control, numbness in the saddle region, rapidly worsening leg weakness, severe unrelenting pain, fever, unexplained weight loss, major trauma, or symptoms suggesting serious medical illness require urgent medical assessment.
What Patients Should Expect From Conservative Care
Patients should not expect that conservative care will erase every degenerative change in the spine. A more realistic goal is to reduce symptoms, improve movement, increase walking tolerance, improve strength, and help the patient function better. Some patients improve quickly, while others need more time. Progress depends on symptom severity, duration, general health, activity level, other joint problems, and consistency with home exercises.
A successful outcome may look different for each person. For one patient, success may mean walking around the block again. For another, it may mean shopping without needing to sit every few minutes. For another, it may mean travelling with less fear of flare-ups. For another, it may mean avoiding or delaying more invasive treatment.
The most helpful approach is usually active and collaborative. The clinician provides assessment, treatment, education, and progression. The patient participates through home exercises, walking practice, pacing strategies, and lifestyle adjustments. Passive treatment alone is rarely enough for long-term improvement.
How The Muscle and Joint Clinic Can Help
At The Muscle and Joint Clinic, our approach to lumbar spinal stenosis is based on understanding the patient’s full presentation. We do not look only at the MRI report or only at the painful area. We assess how the spine, hips, pelvis, legs, nerves, balance, and walking pattern are contributing to the problem.
Treatment may include manual therapy to improve mobility, soft tissue therapy to reduce muscle tension, hip and lumbar mobilization, gentle flexion-biased movement strategies, individualized strengthening, core and glute training, stretching, balance work, and walking progression. Education is also a major part of care. Patients should understand what is happening, what activities are likely to aggravate symptoms, what positions may help, and how to build tolerance safely.
For many patients, the most important part of treatment is creating a realistic plan. A person who has avoided walking for months cannot always jump straight into long walks. A person who flares with standing may need supported exercises first. A person with hip or knee arthritis may need modifications. A person with balance concerns may need a different starting point. The plan should fit the patient.
The Bottom Line
Lumbar spinal stenosis is a common condition that can cause low back pain, buttock pain, leg symptoms, and difficulty walking. It is usually related to age-related narrowing around the nerves in the lower spine. Although the condition is structural, symptoms are influenced by mobility, strength, posture, nerve sensitivity, conditioning, confidence, and activity habits.
The 2019 JAMA Network Open study provides encouraging evidence that nonsurgical care can help patients with lumbar spinal stenosis. All three treatment groups improved over time, especially in walking capacity. Manual therapy combined with individualized exercise produced better short-term improvement at two months, suggesting that a hands-on, personalized rehabilitation approach may be especially useful for patients who are struggling with symptoms and walking limitation.
For patients, the message is hopeful. Lumbar spinal stenosis does not always mean inevitable decline. It does not automatically mean surgery is the only option. With proper assessment, education, manual therapy when appropriate, individualized exercise, and gradual walking progression, many patients can improve their function and regain confidence in daily life.
If you or someone you know has low back, buttock, or leg symptoms that worsen with standing or walking and improve with sitting or leaning forward, lumbar spinal stenosis may be part of the picture. A proper assessment can help determine the cause of symptoms and whether conservative care is appropriate. At The Muscle and Joint Clinic, our goal is to help patients move better, walk farther, and stay active with a plan that is safe, realistic, and individualized.