
Morning or Evening Exercise: Does the Time of Day Really Matter?


Most people think about exercise in terms of what they should do. Should they walk, run, cycle, lift weights, stretch, or do rehabilitation exercises? Others focus on how much they should do. Should they aim for 20 minutes a day, 150 minutes per week, 10,000 steps, or three gym sessions?
These are important questions. The type, intensity, frequency, and consistency of exercise all matter. But research is increasingly asking another question that may be just as important: does the timing of exercise matter?
For many years, the simplest answer has been that the best time to exercise is the time you can actually do consistently. That remains true. A realistic routine that happens regularly is better than a perfect plan that never gets done. However, newer research suggests that the body may respond differently to exercise depending on the time of day, a person’s natural body clock, and their health goals.
This does not mean there is one perfect time for everyone to exercise. It does not mean morning workouts are automatically better. It also does not mean evening exercise is harmful. Instead, the research points toward a more personalized approach. Morning exercise may have certain benefits for sleep timing, fat metabolism, cholesterol, and triglycerides. Evening exercise may have certain benefits for vascular function and blood pressure. Chronotype, which refers to whether someone is naturally more of a morning person or evening person, may also influence how the body responds to exercise.
For patients, this is important because exercise is not just about discipline. It is about matching the right activity, intensity, timing, and recovery strategy to the person in front of us.
The Body Has a Clock
The human body follows internal 24-hour rhythms known as circadian rhythms. These rhythms help regulate sleep and wakefulness, alertness, body temperature, hormone release, digestion, blood sugar regulation, blood pressure, heart rate, and many other physiological functions.
This means the body is not exactly the same at every hour of the day. The way we move, digest food, regulate blood pressure, use energy, and prepare for sleep can vary depending on timing. Melatonin, for example, usually rises in the evening as the body prepares for sleep. Blood pressure and cardiovascular function also follow daily patterns, with certain cardiovascular events being more common at particular times of day (Shen et al., 2025).
Exercise is also a signal to the body clock. Light is the strongest signal for circadian rhythm, but physical activity, meal timing, sleep timing, and daily routines can also influence the body’s rhythm. This is why regular movement at a consistent time may help shape sleep-wake patterns and other health-related rhythms.
In real life, patients often notice this without using scientific language. Some people feel stiff and slow in the morning but much better after moving around for a few hours. Others feel energized early in the day and lose motivation by evening. Some sleep better when they exercise earlier. Others use evening exercise to unwind after work. These differences matter when designing an exercise plan.
What Is Chronotype?
Chronotype refers to a person’s natural tendency to feel more alert and active earlier or later in the day. Morning types often wake up earlier, feel more alert in the first half of the day, and prefer doing demanding tasks in the morning. Evening types often feel more alert later in the day and may find early mornings more difficult. Many people fall somewhere in the middle.
Chronotype is not simply a preference or a personality trait. It reflects how a person’s internal clock aligns with their daily schedule. Two people may complete the same workout at the same intensity, but their bodies may experience that workout differently depending on their chronotype.
This matters because many people are told that the “best” or most disciplined time to exercise is early in the morning. For some people, that works very well. They feel focused, energetic, and more consistent when they exercise before the day becomes busy. For others, early morning exercise feels unusually difficult. Their body feels stiff, their energy is low, their heart rate may climb faster, and they may struggle to stay consistent.
That does not mean they are lazy. It may mean that their exercise timing does not match their biology, their sleep schedule, or their recovery needs.
Study One: Exercise Timing, Chronotype, and Fuel Use
A 2025 study by Kang and colleagues examined how exercise timing and chronotype influence cardiorespiratory and metabolic responses during aerobic exercise. The study included 30 healthy young adults, including 15 men and 15 women. Participants were categorized as morning types, neither types, or evening types using the Morningness-Eveningness Questionnaire (Kang et al., 2025).
Each participant completed two treadmill exercise sessions. One session was performed in the morning before 9:00 AM, and the other was performed in the afternoon after 3:00 PM. Both sessions involved 30 minutes of aerobic exercise at approximately 75% of VO₂max. The researchers measured oxygen uptake, heart rate, respiratory exchange ratio, carbohydrate oxidation, and fat oxidation (Kang et al., 2025).
In simpler terms, the researchers wanted to know whether the body uses energy differently during morning versus afternoon exercise and whether a person’s chronotype changes the body’s response.
The study found no major difference in oxygen uptake or heart rate between morning and afternoon exercise overall. This suggests that, at least for submaximal aerobic exercise in healthy young adults, the basic cardiorespiratory demand of the workout may not change dramatically based on whether it is done in the morning or afternoon.
However, the study did find differences in fuel use. Morning exercise was associated with a lower respiratory exchange ratio and lower carbohydrate oxidation compared with afternoon exercise. Fat oxidation was also higher in the morning, although this was described as a trend rather than a statistically significant finding (Kang et al., 2025).
This suggests that morning aerobic exercise may encourage the body to rely slightly more on fat as a fuel source during the workout. This does not mean that morning exercise automatically causes fat loss. Fat loss is influenced by total weekly activity, diet, sleep, stress, muscle mass, hormones, and overall energy balance. Still, the finding is useful because it suggests that the body’s metabolism may respond differently depending on exercise timing.
Chronotype May Affect Heart Rate During Exercise
One of the most interesting findings from Kang et al. was that heart rate during exercise differed across chronotypes. Evening types had the highest exercising heart rates, neither types were in the middle, and morning types had the lowest heart rates. This occurred even though the groups were similar in aerobic fitness and other baseline characteristics (Kang et al., 2025).
This is clinically important because heart rate is one way the body shows how hard it is working. If an evening-type person has a higher heart rate response during exercise, especially when exercising at a time that does not match their natural rhythm, the same workout may feel more demanding.
This does not mean evening types should avoid morning exercise. It means exercise prescription should be individualized. If someone feels unusually strained during early morning exercise, it may be helpful to adjust the warm-up, lower the intensity, monitor heart rate, or consider a later exercise window.
This is especially relevant for patients recovering from pain or injury. A person with low back pain, knee arthritis, shoulder pain, tendon irritation, or general morning stiffness may not tolerate a demanding early morning workout. The exercise itself may be appropriate, but the timing and intensity may need to be adjusted.
Study Two: Morning Versus Evening Exercise Over 12 Weeks
A second important study was published in Scientific Reports by Shen and colleagues in 2025. This randomized controlled trial compared the effects of 12 weeks of morning versus evening aerobic exercise on sleep, lipid profiles, body composition, and vascular function (Shen et al., 2025).
The study included 58 sedentary young adult males between the ages of 18 and 28. Participants were divided into three groups: a morning exercise group that trained between 6:00 and 8:00 AM, an evening exercise group that trained between 6:00 and 8:00 PM, and a control group that did not exercise (Shen et al., 2025).
The exercise program lasted 12 weeks. Participants completed at least three sessions per week and accumulated at least 150 minutes of moderate-intensity aerobic exercise weekly. Activities included running, jumping rope, elliptical training, and cycling. Exercise intensity was monitored using heart rate, with a target intensity of 60% to 70% of heart rate reserve (Shen et al., 2025).
This study is helpful because it did not only look at one workout. It examined what happened after a structured training program. It also measured several outcomes that matter to patients, including sleep timing, melatonin rhythm, body fat, cholesterol, triglycerides, resting heart rate, blood pressure, and carotid artery blood flow.
Morning Exercise and Sleep Timing
Sleep was one of the major outcomes in the Shen et al. study. The researchers used the Munich ChronoType Questionnaire to assess sleep patterns and also measured dim light melatonin onset, known as DLMO. DLMO is a common biological marker used to estimate circadian timing because it reflects when melatonin begins to rise under dim light conditions (Shen et al., 2025).
After 12 weeks, both the morning and evening exercise groups showed reduced sleep latency. Sleep latency refers to how long it takes to fall asleep after going to bed. In other words, regular aerobic exercise helped participants fall asleep faster, regardless of whether they exercised in the morning or evening (Shen et al., 2025).
However, morning exercise had a more specific effect on sleep timing. The morning exercise group showed an advance in sleep onset, mid-sleep time, sleep end time, and DLMO. This means their sleep-wake rhythm shifted earlier. Their biological night appeared to begin earlier, and their sleep schedule moved earlier as well (Shen et al., 2025).
This may be relevant for people who struggle with late bedtimes, delayed sleep schedules, or difficulty waking in the morning. Morning exercise, especially when combined with morning light exposure, may help reinforce an earlier sleep-wake rhythm. It should not be viewed as a cure for insomnia or sleep disorders, but it may be a useful lifestyle strategy for certain patients.
This is also relevant in musculoskeletal care. Poor sleep can increase pain sensitivity, reduce recovery, affect mood, and make exercise harder to maintain. When patients are dealing with low back pain, neck pain, headaches, tendon pain, or arthritis, sleep quality often plays an important role in how well they recover.
Morning Exercise and Metabolic Health
The Shen et al. study also found that both morning and evening exercise reduced body fat after 12 weeks. However, the morning exercise group showed significant reductions earlier, with measurable changes as early as week four. Morning exercise was also associated with reductions in total cholesterol and triglycerides. The evening exercise group did not show the same lipid changes in this study (Shen et al., 2025).
This fits with the Kang et al. study, which found that morning aerobic exercise may shift fuel use toward greater fat oxidation during the exercise session (Kang et al., 2025). Taken together, these studies suggest that morning exercise may have particular benefits for fat metabolism and lipid regulation in some populations.
However, this should be interpreted carefully. Shen et al. studied young sedentary males with normal body mass index and without major cardiovascular or metabolic disease. The results may not apply the same way to older adults, women, people with diabetes, people with obesity, people with shift-work schedules, or people with cardiovascular disease.
The better takeaway is not that morning exercise is always superior for metabolism. The better takeaway is that exercise timing may influence metabolic outcomes, and the best timing may depend on the individual’s health status, sleep rhythm, goals, and ability to stay consistent.
Study Three: UK Biobank, Peak Activity Timing, and Cardiovascular Mortality
The third study adds a longer-term population-level perspective. Ma and colleagues examined the association between the time of day of peak physical activity and cardiovascular mortality using data from the UK Biobank (Ma et al., 2023).
This was not a short exercise trial. It was a large observational cohort study involving 94,489 adults with objectively measured physical activity. Participants wore accelerometers, which allowed researchers to examine when during the day their physical activity tended to peak. The researchers categorized peak physical activity timing into early morning, late morning, midday, and night. The midday group was used as the reference group (Ma et al., 2023).
During a median follow-up of 6.9 years, the researchers identified 629 cardiovascular deaths. Compared with the midday peak activity group, the early morning peak activity group had a higher hazard of cardiovascular mortality, and the night peak activity group also had a higher hazard. The late morning group did not show the same statistically significant increase compared with midday (Ma et al., 2023).
At first glance, this may sound surprising. Many people assume early morning activity is always healthier. However, the study is not saying that a morning walk is dangerous or that people should avoid moving early in the day. It is saying that, in this large population, having peak physical activity in the early morning or at night was associated with higher cardiovascular mortality compared with having peak activity around midday.
This is an association, not proof of cause and effect. Observational studies can show patterns, but they cannot prove that the timing itself caused the increased risk. People who are most active very early or late may differ in other ways. They may have different work schedules, sleep patterns, health conditions, stress levels, medication use, shift-work exposure, or lifestyle factors. Even with statistical adjustments, some residual confounding is always possible.
Still, the study is important because it supports the broader idea that timing may matter. The cardiovascular system follows circadian patterns, and physical activity performed at different times of day may interact with those patterns.
Chronotype Changed the Pattern in the UK Biobank Study
One of the most interesting parts of the Ma et al. study was the chronotype-stratified analysis. The researchers found that the increased cardiovascular mortality seen in the early morning peak activity group was mainly observed in evening-type participants. In contrast, the increased cardiovascular mortality seen in the night peak activity group was mainly observed in morning-type participants (Ma et al., 2023).
This suggests that mismatch may matter. An evening-type person whose peak activity occurs very early in the morning may be exercising at a time that is misaligned with their natural rhythm. Similarly, a morning-type person whose peak activity occurs at night may be active at a time that is misaligned with their body clock.
This does not prove that chronotype mismatch causes cardiovascular mortality. But it fits with the broader theme seen in other studies: the timing of exercise may not have the same effect for everyone.
For patients, this is a helpful concept. The goal is not to force everyone into the same exercise schedule. The goal is to find a routine that supports the person’s health, recovery, sleep, and consistency.
How Should We Interpret These Studies Together?
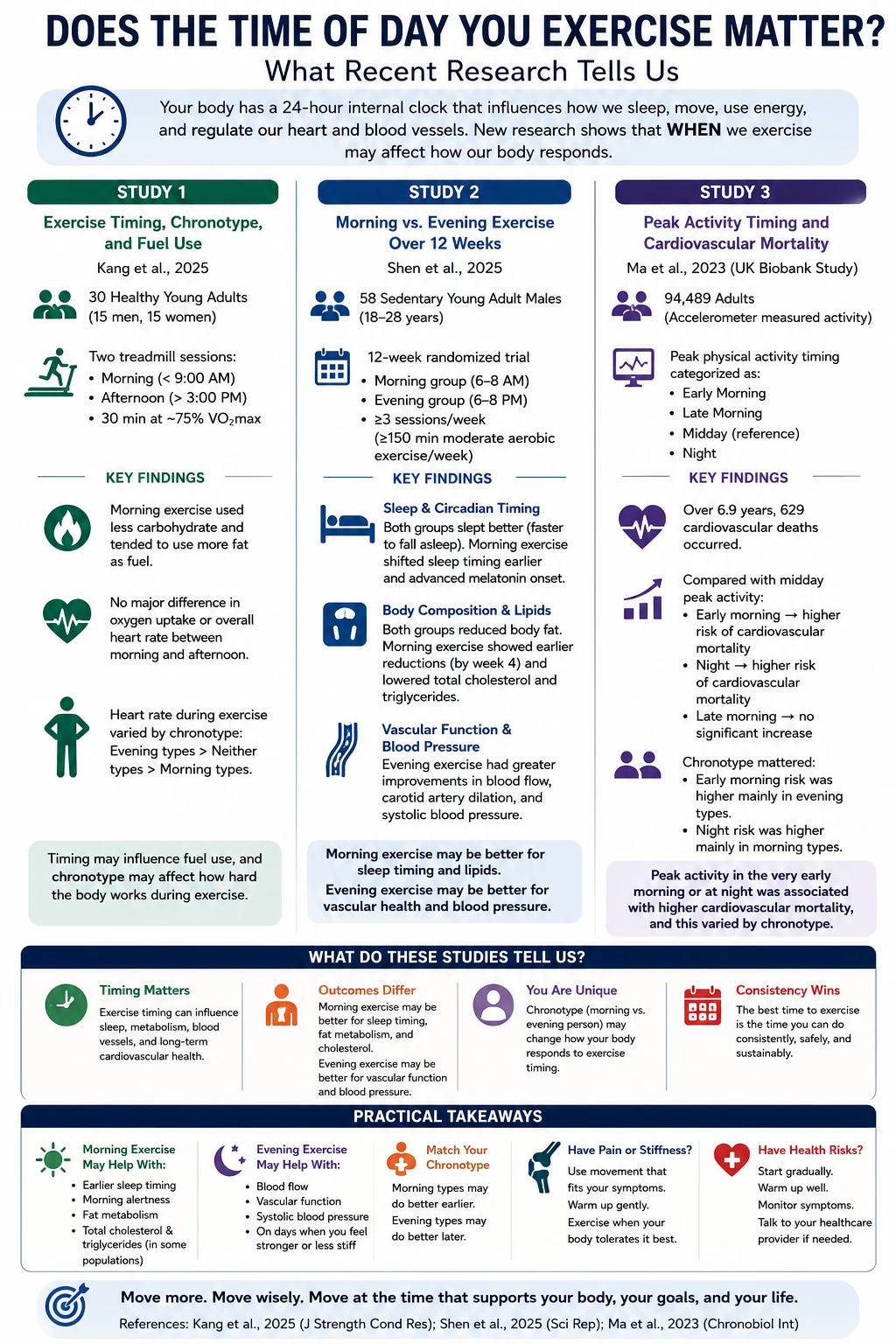
When we look at Kang et al., Shen et al., and Ma et al. together, a more complete picture begins to emerge.
Kang et al. showed that morning aerobic exercise may influence fuel use during a workout, with lower carbohydrate oxidation and a trend toward higher fat oxidation. The study also suggested that chronotype may influence heart rate responses during exercise (Kang et al., 2025).
Shen et al. showed that 12 weeks of aerobic exercise improved health in both morning and evening exercise groups. Morning exercise appeared more effective for advancing sleep timing, improving sleep rhythm, reducing body fat earlier, and lowering total cholesterol and triglycerides. Evening exercise appeared more effective for improving certain vascular function measures and systolic blood pressure (Shen et al., 2025).
Ma et al. showed that, in a large UK Biobank cohort, peak activity timing was associated with cardiovascular mortality, and that the relationship differed by chronotype. Early morning peak activity appeared more concerning in evening types, while night peak activity appeared more concerning in morning types (Ma et al., 2023).
Together, these studies do not give us one universal answer. Instead, they suggest that exercise timing may be outcome-specific and person-specific.
If the goal is sleep timing, morning exercise may be useful. If the goal is lipid regulation or body fat reduction, morning exercise may have advantages in some populations. If the goal is vascular function or blood pressure regulation, evening exercise may have advantages in some populations. If the person is clearly a morning type or evening type, matching exercise timing to chronotype may improve tolerance and possibly health response.
What This Means for the Average Patient
For most people, the first priority is simply to move more. Exercise has well-established benefits for cardiovascular health, metabolic health, mental health, musculoskeletal health, pain management, strength, mobility, and quality of life. A person who walks consistently in the evening is likely doing far more for their health than someone who plans to exercise every morning but rarely follows through.
However, once a person is ready to build a routine, timing can be used strategically.
Morning exercise may be helpful for people who want to create a consistent routine before the day gets busy. It may also be helpful for people who want to shift their sleep schedule earlier or improve morning alertness. Based on the research above, morning aerobic exercise may also be useful for people focused on body composition or certain lipid markers, although this should not be overstated.
Evening exercise may be helpful for people who feel stronger, looser, and more coordinated later in the day. It may be a better fit for those who feel too stiff in the morning or who struggle to exercise before work or school. Evening exercise may also have benefits for vascular function and systolic blood pressure, based on the Shen et al. findings.
Midday or late morning exercise may be a useful option for many people as well. The Ma et al. UK Biobank study used midday as the reference group and found that early morning and night peak activity were associated with higher cardiovascular mortality compared with midday (Ma et al., 2023). This does not mean midday is automatically the safest or best time for everyone, but it does suggest that moderate timing may be worth considering, especially for people who feel poorly exercising at the extremes of the day.
What About People With Pain or Stiffness?
Exercise timing is especially important for people with musculoskeletal pain. Many painful conditions fluctuate throughout the day. A person with osteoarthritis may feel stiff in the morning and better after gentle movement. A person with low back pain may feel worse after prolonged sitting and better after walking. A person with tendon pain may tolerate loading exercises better at certain times of day. A person with neck pain or headaches may notice symptoms change depending on sleep, posture, stress, and work schedule.
This is why rehabilitation should be individualized. The same exercise can feel very different depending on when it is performed. A strengthening exercise that feels too difficult at 6:30 AM may feel much more manageable at 4:00 PM. A mobility routine may be useful in the morning, while more demanding strengthening may be better later in the day.
At The Muscle and Joint Clinic, we often encourage patients to think of exercise timing as part of the prescription. The exercise itself matters, but so does the dosage, intensity, warm-up, recovery period, and time of day.
For a patient with morning low back stiffness, it may be better to start with gentle walking, breathing, and mobility in the morning, then complete strengthening exercises later in the day. For a patient with knee arthritis, a morning mobility routine may help reduce stiffness, while strength work may be better tolerated once the body has warmed up. For a patient with tendon pain, loading exercises may need to be scheduled when symptoms are calm and recovery time is available afterward.
The goal is not just to exercise. The goal is to exercise in a way the body can adapt to.
The Problem With “One-Size-Fits-All” Exercise Advice
The biggest mistake in exercise advice is assuming that everyone should follow the same routine. Some people do very well with early morning exercise. Others do not. Some people sleep perfectly after evening exercise. Others feel wired and have trouble falling asleep. Some people feel strongest later in the day. Others lose motivation if they wait too long.
Research on exercise timing supports what clinicians often see in practice: the best plan is the one that matches the person.
This matters because guilt and shame are common barriers to exercise. People may think they are failing because they cannot wake up at 5:00 AM to train. But if they are naturally an evening type, sleep poorly, feel stiff in the morning, or have pain that improves later in the day, an early morning workout may not be the best starting point.
A better approach is to ask: When does your body feel most ready to move? When are you most consistent? When does exercise improve your energy instead of draining it? When does it support your sleep instead of disrupting it? When do your symptoms tolerate it best?
Those answers are often more useful than generic advice.
Practical Guidance: How to Choose Your Exercise Time
If your goal is consistency, choose the time you are most likely to follow through. For many people, this is the most important factor. Consistency drives long-term benefits.
If your goal is improving sleep timing, morning exercise may be helpful, especially when combined with morning light exposure and a regular wake time. This may be particularly useful for people who tend to fall asleep too late or struggle to shift their sleep schedule earlier.
If your goal is body composition or lipid health, morning aerobic exercise may have advantages in some people, based on the findings from Kang et al. and Shen et al. However, nutrition, total weekly exercise volume, resistance training, sleep, and stress management remain essential.
If your goal is blood pressure or vascular function, evening aerobic exercise may have potential advantages, based on the Shen et al. study. This should be individualized, especially for people with cardiovascular conditions or those taking blood pressure medication.
If you are a morning type, you may tolerate earlier activity better. If you are an evening type, you may tolerate later activity better. If your schedule forces you to exercise at a time that does not match your chronotype, adjust the intensity and warm-up accordingly.
If you have pain or stiffness, do not judge your body based only on the first few minutes of movement. Many people need a gradual warm-up. Start gently, increase slowly, and pay attention to whether symptoms improve, stay stable, or worsen.
What These Studies Do Not Prove
It is important to be balanced. Kang et al. studied only 30 healthy young adults, and the morning-type and evening-type groups were small. Shen et al. studied 58 sedentary young adult males and did not include women, older adults, shift workers, or people with major cardiovascular or metabolic disease. Ma et al. was a large observational study, but observational research cannot prove cause and effect.
This means we should not overstate the findings. The evidence does not prove that one exercise time is best for everyone. It does not prove that morning exercise is always better for metabolism or that evening exercise is always better for blood pressure. It also does not prove that early morning or night exercise directly causes cardiovascular mortality.
What the evidence does suggest is that timing may matter, chronotype may matter, and personalization may improve exercise tolerance and health outcomes.
The Bottom Line
The best time to exercise is still the time you can do consistently, safely, and sustainably.
But timing may matter more than we used to think.
Morning exercise may help shift the sleep-wake cycle earlier, improve sleep timing, support fat metabolism, and improve certain lipid markers in some people. Evening exercise may improve vascular function and systolic blood pressure in some people. Large observational data suggest that peak activity timing may be associated with cardiovascular mortality, and that mismatch between activity timing and chronotype may be important.
The key message is not that everyone should exercise at the same time. The key message is that exercise should be personalized.
If morning exercise helps you stay consistent and feel better, it may be a great choice. If evening exercise helps you move better, train harder, and stick with the routine, that may be the better option. If you are recovering from pain or injury, the right time may be the time your body tolerates movement best. If you have cardiovascular risk factors, the plan should be gradual, appropriate, and discussed with a healthcare professional when needed.
At The Muscle and Joint Clinic, we help patients build exercise and rehabilitation plans that fit their body, their schedule, their goals, and their recovery. Whether the goal is to reduce pain, improve mobility, build strength, return to sport, or improve overall health, the right plan should work with your body, not against it.
Disclaimer: This article is for general educational purposes only and is not intended to provide medical advice, diagnosis, or treatment. The research discussed in this article should be interpreted in context, as exercise timing may affect individuals differently depending on age, health history, fitness level, sleep schedule, chronotype, medications, symptoms, and personal goals. If you have chest pain, dizziness, unexplained shortness of breath, high blood pressure, diabetes, cardiovascular disease, or any other medical condition, please speak with a qualified healthcare provider before starting or changing an exercise program. If you are recovering from an injury or experiencing pain with exercise, an individualized assessment can help determine what type, intensity, and timing of exercise is most appropriate for you.
References
Kang, J., Ratamess, N. A., Faigenbaum, A. D., Bush, J. A., Fardman, B., Vargas, A., Andriopoulos, T., Melao, J., O’Connell, E., Duff, A., Cmielewski, A., DeSalvo, J., Johnson, A., & Watts, M. (2025). Unlocking the body’s clock: The role of exercise timing and chronotype in cardiometabolic responses. Journal of Strength and Conditioning Research, 39(6), 634–641.
Ma, T., Jennings, L., Sirard, J. R., Xie, Y. J., & Lee, C. D. (2023). Association of the time of day of peak physical activity with cardiovascular mortality: Findings from the UK Biobank study. Chronobiology International, 40(3), 324–334. doi:10.1080/07420528.2023.2170240
Shen, B., Zheng, H., Liu, H., Chen, L., & Yang, G. (2025). Differential benefits of 12-week morning vs. evening aerobic exercise on sleep and cardiometabolic health: A randomized controlled trial. Scientific Reports, 15, 18298. doi:10.1038/s41598-025-02659-8
Vitale, J. A., & Weydahl, A. (2017). Chronotype, physical activity, and sport performance: A systematic review. Sports Medicine, 47, 1859–1868.
World Health Organization. (2020). WHO guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine, 54(24), 1451–1462.