
Spinal Stenosis Explained
What It Is, What the Research Says, and How Our Clinic Can Help


Spinal stenosis is a term many people hear only after months of back pain, leg heaviness, or difficulty walking. By the time the diagnosis is mentioned, patients are often already worried about surgery, permanent nerve damage, or whether they will ever get back to normal activity. Those concerns are understandable. The phrase itself sounds serious, and the symptoms can be frustrating. But a diagnosis of spinal stenosis does not automatically mean surgery is the only option, and it does not mean that nothing can be done. In fact, a large part of the research on lumbar spinal stenosis supports starting with conservative care for many patients, especially when symptoms are mild to moderate and there are no urgent neurologic red flags (Katz et al., 2022; Webb et al., 2024).
At the Muscle and Joint Clinic, one of the most important parts of care is helping patients understand what spinal stenosis actually is, why it causes the symptoms it does, and what evidence-based treatment can realistically achieve. For many people, the biggest goals are simple and meaningful: walk farther, stand longer, sleep better, move with less fear, and avoid the cycle of pain and inactivity that can slowly shrink daily life. Those goals matter, and research suggests they are often worth working toward with a structured, individualized rehabilitation approach before moving to more invasive options (Schneider et al., 2019; Iversen et al., 2010).
What is spinal stenosis?
Spinal stenosis means there is a narrowing in one or more spaces around the nerves of the spine. When this happens in the lower back, it is called lumbar spinal stenosis, and that is the form most people mean when they talk about spinal stenosis causing pain into the buttocks or legs. The narrowing can happen in the central canal, the lateral recesses, or the openings where the nerves travel out of the spine, called the foramina (Katz et al., 2022; Webb et al., 2024).
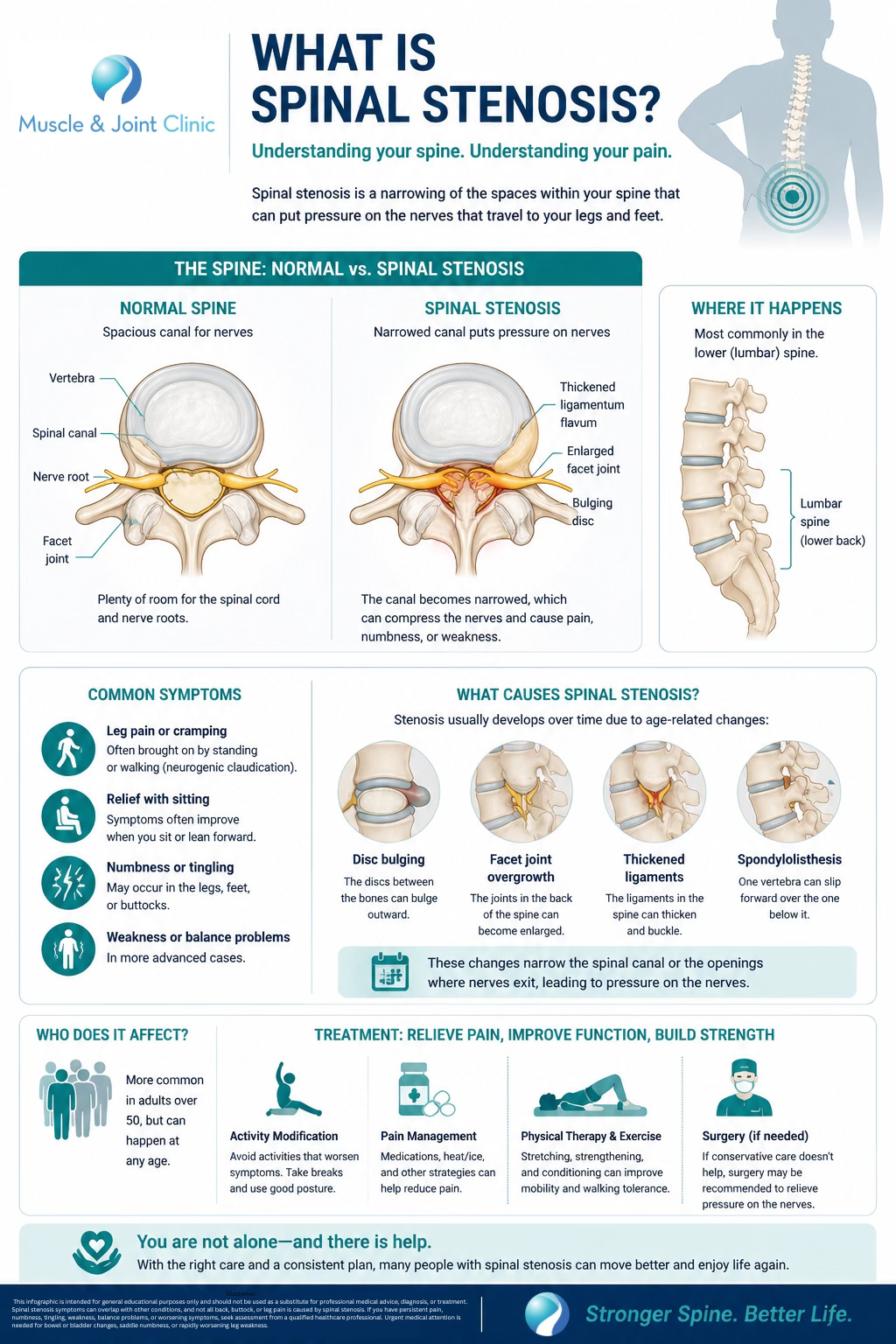
In most adults, lumbar spinal stenosis is not caused by one dramatic event. It is usually a degenerative condition, meaning it develops gradually over time as the spine changes with age. Discs can lose height and bulge. Facet joints can enlarge and become arthritic. Ligaments such as the ligamentum flavum can thicken. Bone spurs can develop. In some people, one vertebra may shift slightly relative to another, a condition called spondylolisthesis, which can add to the narrowing (Webb et al., 2024; Katz et al., 2022). None of these changes are unusual in aging spines, but in some people they become significant enough to crowd the nerves and create symptoms.
That point is important, because many people have narrowing on imaging and no symptoms at all. Research has shown that imaging findings and symptoms do not always match perfectly. In other words, the scan matters, but the clinical story matters too. Treatment should be guided by both (Katz et al., 2022).
Why does spinal stenosis cause pain, heaviness, or numbness in the legs?
Lumbar spinal stenosis is most famous for a symptom pattern called neurogenic claudication. That sounds technical, but the pattern is often very recognizable. People may feel aching, cramping, burning, tingling, numbness, fatigue, or heaviness in the buttocks and legs, sometimes with low back pain and sometimes with leg symptoms that are more bothersome than the back itself. These symptoms are often made worse by standing upright or walking, and relieved by sitting, bending forward, or leaning over something such as a shopping cart (Katz et al., 2022; Webb et al., 2024).
The reason is mechanical. Extension, or arching backward, tends to reduce the available space in the canal and foramina. Flexion, or bending forward, tends to increase it. That is why many patients say they can walk farther while leaning on a cart than they can while standing fully upright. It is also why cycling is often easier to tolerate than walking for some people with spinal stenosis: the flexed posture can reduce symptom provocation (Iversen et al., 2010; Katz et al., 2022).
The exact mechanism of symptoms is still not fully settled. The narrowing may mechanically compress nerves, reduce blood supply, impair venous drainage, or create a combination of local inflammatory and ischemic effects around nerve roots. Clinically, though, the result is familiar: standing and walking become harder, while sitting often feels like relief (Katz et al., 2022).
What does spinal stenosis usually feel like?
Most patients do not walk in and say, “I think I have neurogenic claudication.” They say things like:
“My legs get heavy when I walk.”
“I can only stand for a few minutes before I need to sit.”
“My back is stiff, but it’s really the buttocks and legs that stop me.”
“I feel better leaning forward.”
“My walking tolerance is getting worse.”
Those descriptions fit the research surprisingly well. Lumbar spinal stenosis often presents with back and lower-extremity discomfort that worsens with prolonged standing and walking and improves with sitting or flexion-based positions (Katz et al., 2022; Webb et al., 2024). Symptoms may be bilateral, though not always. Some patients also report balance problems, unsteadiness, or a wide-based gait, especially as the condition progresses (Katz et al., 2022).
Not every case looks identical. Some people have more pain, others more numbness or fatigue. Some mainly notice reduced walking distance. Some have symptoms only with faster walking or hills. Others struggle even with shopping or household tasks. This is one reason an individualized assessment matters. A label alone does not tell the whole story.
How is spinal stenosis diagnosed?
A proper diagnosis is based on symptoms, examination findings, and imaging, not imaging alone. MRI is generally considered the preferred imaging study because it provides a detailed view of the spinal canal, nerve spaces, discs, ligaments, and surrounding tissues (Katz et al., 2022; Webb et al., 2024). CT may be used when MRI is not appropriate.

Clinically, providers often look for the combination of leg-dominant symptoms, worse with walking or standing, improved with flexion or sitting, and a scan showing narrowing that makes sense with the patient’s presentation. On examination, a clinician may assess walking tolerance, balance, lumbar extension tolerance, neurologic function, lower-extremity strength, reflexes, sensation, hip mobility, and possible competing diagnoses such as vascular claudication, hip osteoarthritis, sacroiliac pain, or peripheral neuropathy (Webb et al., 2024).
This distinction matters because not all leg pain with walking is stenosis. The differential diagnosis can include vascular claudication, hip pathology, nerve root impingement from disc herniation, piriformis-related pain, sacroiliac dysfunction, and more (Webb et al., 2024). That is why assessment should be thorough rather than based only on a scan report.
Certain symptoms require urgent medical attention. Bowel or bladder changes, saddle numbness, or rapidly progressive leg weakness may indicate significant nerve compression such as cauda equina syndrome and should not be managed as routine spinal stenosis (Katz et al., 2022; Webb et al., 2024).
What does the research say about the best treatment?
The overall research message is more hopeful than many patients expect. Major reviews and guidelines generally support conservative care as the first-line approach for many people with lumbar spinal stenosis, especially when symptoms are bothersome but not acutely progressive neurologically (Katz et al., 2022; Webb et al., 2024).
A 2022 JAMA review concluded that first-line therapy includes activity modification, analgesia, and physical therapy, and noted that long-term benefits of epidural steroid injections have not been clearly demonstrated (Katz et al., 2022). The 2024 American Family Physician review similarly recommended nonoperative treatment first in the absence of urgent findings, with NSAIDs considered first-line medication options when appropriate, and surgery reserved for cases where conservative care fails or neurologic symptoms worsen (Webb et al., 2024).
That does not mean surgery has no role. It does. But it means many patients should not assume they must jump straight to an operation simply because the MRI says “stenosis.” Research suggests there is meaningful room for rehabilitation and symptom improvement before that point (Schneider et al., 2019; Katz et al., 2022).
Do people actually improve without surgery?
Often, yes. One of the common fears around spinal stenosis is that it only gets worse. The truth is more nuanced. Lumbar spinal stenosis is degenerative, but symptoms do not always deteriorate in a straight line. Some people worsen, many remain stable, and some improve with nonsurgical treatment (Katz et al., 2022). That matters, because it supports the idea that a well-designed rehabilitation plan is not just “delaying the inevitable.” For many patients, it is a meaningful treatment path in its own right.
A useful example comes from Schneider and colleagues’ randomized clinical trial, which compared medical care, group exercise, and manual therapy plus individualized exercise in 259 older adults with lumbar spinal stenosis. All three groups improved in walking capacity over time. The manual therapy plus individualized exercise group had better short-term improvement at two months in symptoms, physical function, and walking capacity compared with the other groups. By six months, the differences between groups were no longer statistically significant, but the walking gains across all groups remained important (Schneider et al., 2019). That tells us two things: first, nonsurgical care can help; and second, a more tailored rehab approach may offer stronger early gains.
What kind of exercise helps spinal stenosis?
Exercise for spinal stenosis is not about forcing through pain or doing generic “back exercises.” The best evidence supports structured, targeted programs that match the way symptoms behave.
The 2010 review by Iversen and colleagues found that therapeutic exercise and manual therapy generally produced small-to-moderate benefits in pain, disability, and function in patients with mild to moderate lumbar spinal stenosis. Importantly, the better results tended to come from combined programs, not a single isolated exercise. Aerobic activity, flexibility work, strengthening, stabilization, and manual therapy often worked better together than when used alone (Iversen et al., 2010).
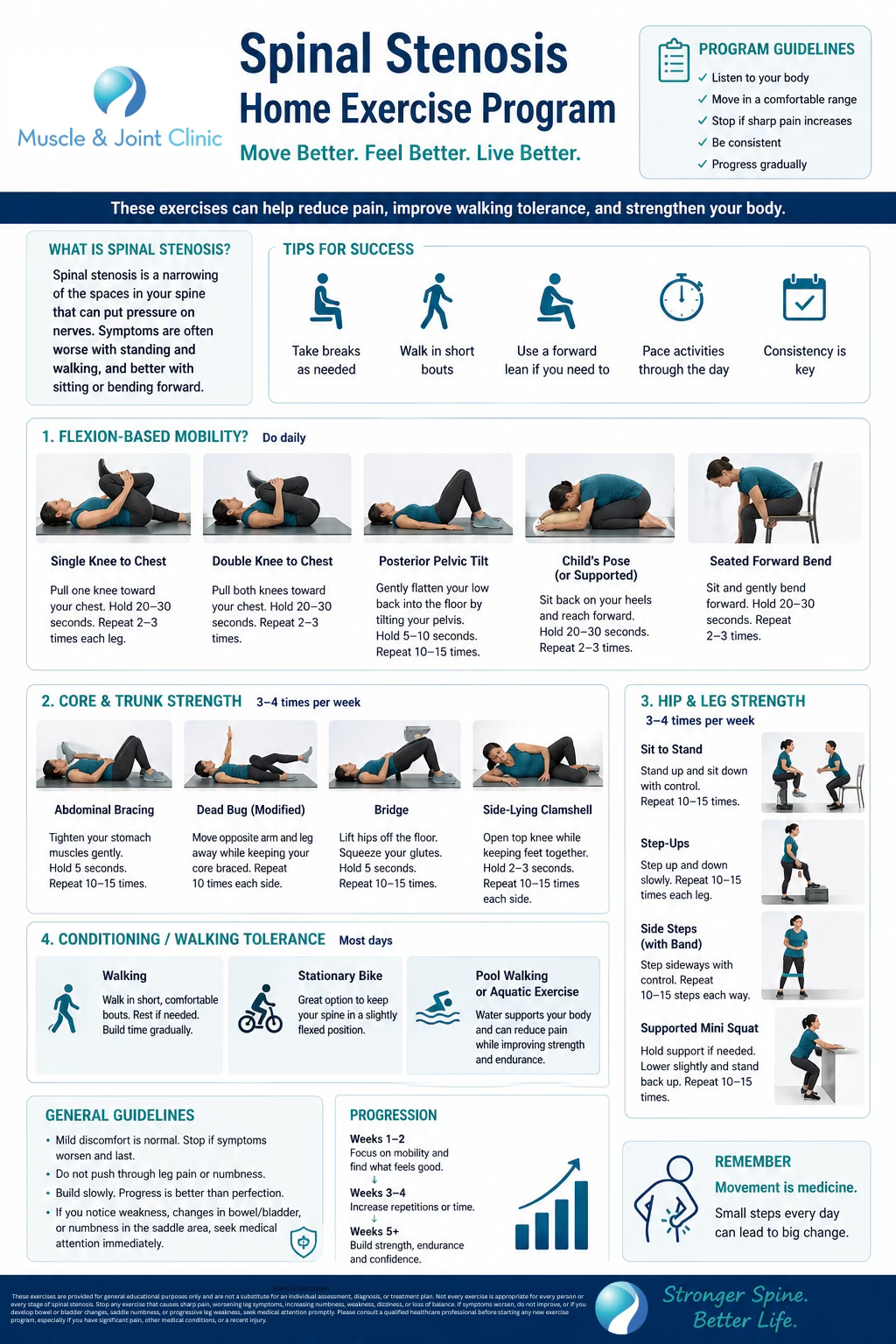
This lines up with more recent clinical thinking. In practice, good rehab programs often include:
education on symptom triggers and pacing
flexion-biased movements when appropriate
trunk and hip strengthening
mobility work for the lumbar spine, hips, and lower limbs
walking progression or conditioning
cycling or similar aerobic exercise that is easier to tolerate
manual therapy as an adjunct, not as the whole plan
Cycling is often better tolerated than walking because it keeps the spine in a more flexed position (Iversen et al., 2010). Supported treadmill walking, home exercise, and structured strengthening can also help. The key is not one magical exercise. The key is an individualized progression.
What about manual therapy?
Manual therapy is sometimes misunderstood as either a miracle solution or something that does nothing. The evidence suggests a more realistic middle ground. When combined with individualized exercise, manual therapy may provide helpful short-term improvement in symptoms and physical function for some patients with lumbar spinal stenosis (Schneider et al., 2019; Iversen et al., 2010).
This does not mean hands-on care alone is the answer. In fact, the stronger studies used manual therapy as part of a broader active treatment plan. That is how we view it clinically as well. Manual therapy may help reduce stiffness, improve tolerance to movement, address surrounding joint and soft tissue restrictions, and create a better starting point for exercise. But it works best when it is paired with a progressive plan aimed at walking tolerance, strength, function, and self-management.
When is surgery considered?
Surgery enters the conversation when symptoms remain meaningfully limiting despite a reasonable course of conservative care, or when neurologic issues are progressing. Decompression surgery can be effective in selected patients, particularly when leg symptoms and walking limitation are substantial (Katz et al., 2022; Webb et al., 2024).
Fusion may sometimes be discussed when there is instability, spondylolisthesis, or other complicating factors, but the indications are not always straightforward. Fusion generally carries greater cost, greater operative burden, and higher complication risk than decompression alone, so it should be considered carefully (Katz et al., 2022).
The practical takeaway for patients is not “avoid surgery at all costs.” It is “do not assume surgery is the first step for everyone.” Many patients deserve a thorough, evidence-based conservative trial first.
How our clinic helps patients with spinal stenosis
At the Muscle and Joint Clinic, our role is not just to identify spinal stenosis. It is to help patients understand how it is affecting their movement, walking, confidence, and daily function, and then build a plan that actually matches those problems.
That starts with a detailed assessment. We look at symptom behavior, walking tolerance, posture, balance, spinal and hip mobility, strength, neurologic findings, and the tasks that matter most to the patient. We also review imaging in context. A report that says “multilevel degenerative changes” only becomes useful when connected to the actual clinical picture.
From there, treatment is individualized. Depending on the patient, care may include physiotherapy-guided exercise, flexion-biased movement strategies, hip and core strengthening, manual therapy, gait and walking progression, mobility work, home exercise coaching, and education on pacing and flare-up management. Some patients benefit from a chiropractic component within a broader rehab plan. Others are better served primarily through physiotherapy-led rehabilitation. What matters most is matching the plan to the patient rather than forcing the patient into a fixed protocol.
We also help patients know when conservative care is working and when the plan needs adjustment. If symptoms are not progressing as expected, if walking tolerance continues to decline, or if neurologic signs become more concerning, we can help guide referral for further medical workup, imaging, injection consultation, or surgical opinion when necessary.
What should patients remember?
The main message from the research is this: spinal stenosis is common, often manageable, and not automatically a surgical condition. Conservative care, particularly structured exercise-based rehabilitation, can improve pain, disability, and walking tolerance for many patients (Katz et al., 2022; Webb et al., 2024; Schneider et al., 2019; Iversen et al., 2010).
A combined program that includes aerobic conditioning, flexibility, strengthening, and individualized hands-on care may offer the strongest short-term improvement, especially in walking and function (Schneider et al., 2019; Iversen et al., 2010). Not every patient will respond the same way, and some will eventually need surgery, but many patients benefit from starting with thoughtful, evidence-based conservative care.
If you have been told you have spinal stenosis, or if back and leg symptoms are gradually reducing your walking tolerance and confidence, getting assessed early matters. The right plan can help you move better, do more, and make decisions about next steps from a much stronger position.
References
Iversen, M. D., Choudhary, V. R., & Patel, S. C. (2010). Therapeutic exercise and manual therapy for persons with lumbar spinal stenosis. International Journal of Clinical Rheumatology, 5(4), 425-437.
Katz, J. N., Zimmerman, Z. E., Mass, H., & Makhni, M. C. (2022). Diagnosis and management of lumbar spinal stenosis: A review. JAMA, 327(17), 1688-1699. https://doi.org/10.1001/jama.2022.5921
Schneider, M. J., Ammendolia, C., Murphy, D. R., Glick, R. M., Hile, E., Tudorascu, D. L., Morton, S. C., Smith, C., Patterson, C. G., & Piva, S. R. (2019). Comparative clinical effectiveness of nonsurgical treatment methods in patients with lumbar spinal stenosis: A randomized clinical trial. JAMA Network Open, 2(1), e186828. https://doi.org/10.1001/jamanetworkopen.2018.6828
Webb, C. W., Aguirre, K., & Seidenberg, P. H. (2024). Lumbar spinal stenosis: Diagnosis and management. American Family Physician, 109(4), 350-359.
Disclaimer
This article is for educational purposes only and is not a substitute for individual medical advice, diagnosis, or treatment. If you have bowel or bladder changes, saddle numbness, or rapidly worsening leg weakness, seek urgent medical attention.