
Tension-Type Headaches: Why They Happen and How Chiropractic Care May Help


Headaches are one of the most common reasons people reach for pain medication, push through a difficult workday, avoid exercise, or struggle to concentrate. While there are many different types of headaches, one of the most common is the tension-type headache.
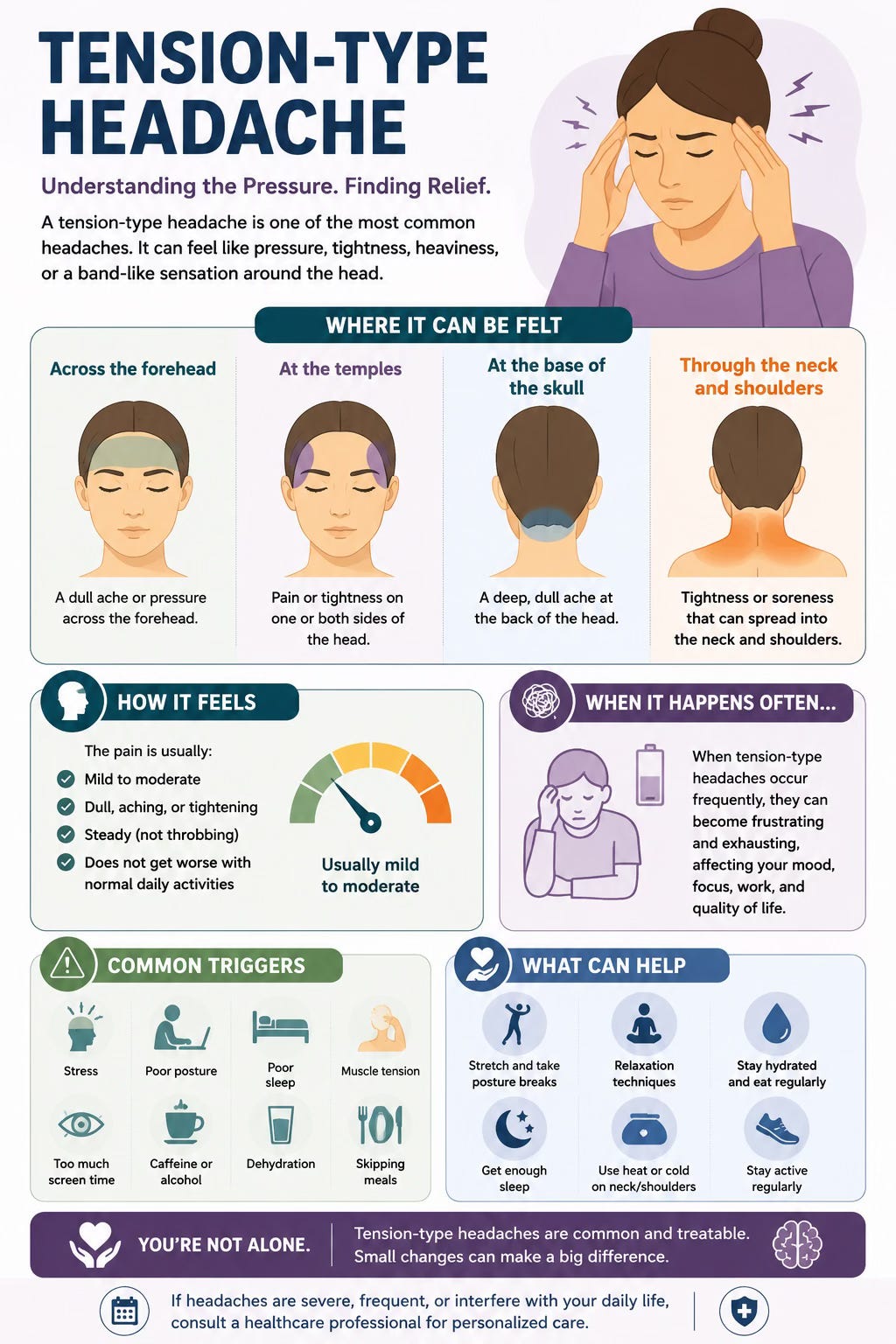
A tension-type headache often feels like pressure, tightness, heaviness, or a band-like sensation around the head. Some people feel it across the forehead or temples. Others feel it at the base of the skull, through the neck, or across the shoulders. The pain is usually mild to moderate, but when it happens often, it can become frustrating and exhausting.
At The Muscle and Joint Clinic, we often see patients who say their headaches build during the day, especially after long hours at a desk, driving, studying, using screens, or going through stressful periods. They may also describe neck tightness, shoulder tension, jaw clenching, poor sleep, or temporary relief with massage, heat, stretching, or movement.
Tension-type headaches are usually not dangerous, but frequent headaches should not be ignored. A headache that keeps returning can affect quality of life, productivity, mood, sleep, and confidence. The goal is not only to reduce pain in the moment, but to understand what may be contributing to the headache pattern and what can be done to reduce its frequency and intensity over time.
What Is a Tension-Type Headache?
A tension-type headache is a primary headache disorder, meaning the headache itself is the condition rather than a symptom of another disease. The International Classification of Headache Disorders describes tension-type headache as usually being bilateral, pressing or tightening in quality, mild to moderate in intensity, and not aggravated by routine physical activity such as walking or climbing stairs (Headache Classification Committee of the International Headache Society, 2018).
Patients often describe it as a tight band around the head, pressure at the temples, heaviness across the forehead, or aching that spreads from the neck to the head. Unlike many migraines, tension-type headaches are usually not strongly throbbing and are less likely to be associated with nausea, vomiting, or major sensitivity to light and sound.
That said, headache patterns can overlap. Some patients have both migraine and tension-type headaches. Others may have headaches that begin with neck and shoulder tension but develop into more migraine-like symptoms. This is why a proper history and assessment matter.
How Common Are Tension-Type Headaches?
Tension-type headaches are very common. Prevalence estimates vary widely depending on how studies define and measure the condition, but research has reported prevalence ranges from approximately 2.2% to 38.3% (Jung et al., 2022; Schwartz et al., 1998). This wide range reflects how differently headache disorders can appear from person to person.
Some people experience tension-type headaches only occasionally. Others have frequent or chronic headaches that become part of their weekly or even daily routine. The more often headaches occur, the more important it becomes to look at contributing factors rather than relying only on short-term pain relief.
Episodic Versus Chronic Tension-Type Headaches
Tension-type headaches are often classified by frequency. Infrequent episodic tension-type headaches occur less than once per month on average. Frequent episodic tension-type headaches occur more often, but fewer than 15 days per month. Chronic tension-type headaches occur on 15 or more days per month for more than three months (Headache Classification Committee of the International Headache Society, 2018).
This distinction is important because occasional headaches and chronic headaches are not managed the same way. An occasional headache may improve with rest, hydration, sleep, gentle movement, or occasional medication when appropriate. Frequent or chronic headaches usually require a more complete plan that considers neck function, stress, sleep, workstation habits, exercise, medication use, and possible overlap with migraine or other headache disorders.
What Causes Tension-Type Headaches?
The exact cause of tension-type headaches is not always clear. They are not simply “muscle headaches,” and they are not just stress headaches. Current understanding suggests they involve a combination of nervous system sensitivity, pain processing, muscle tenderness, neck and shoulder tension, lifestyle factors, and sometimes emotional stress (Bendtsen et al., 2010; Headache Classification Committee of the International Headache Society, 2018).
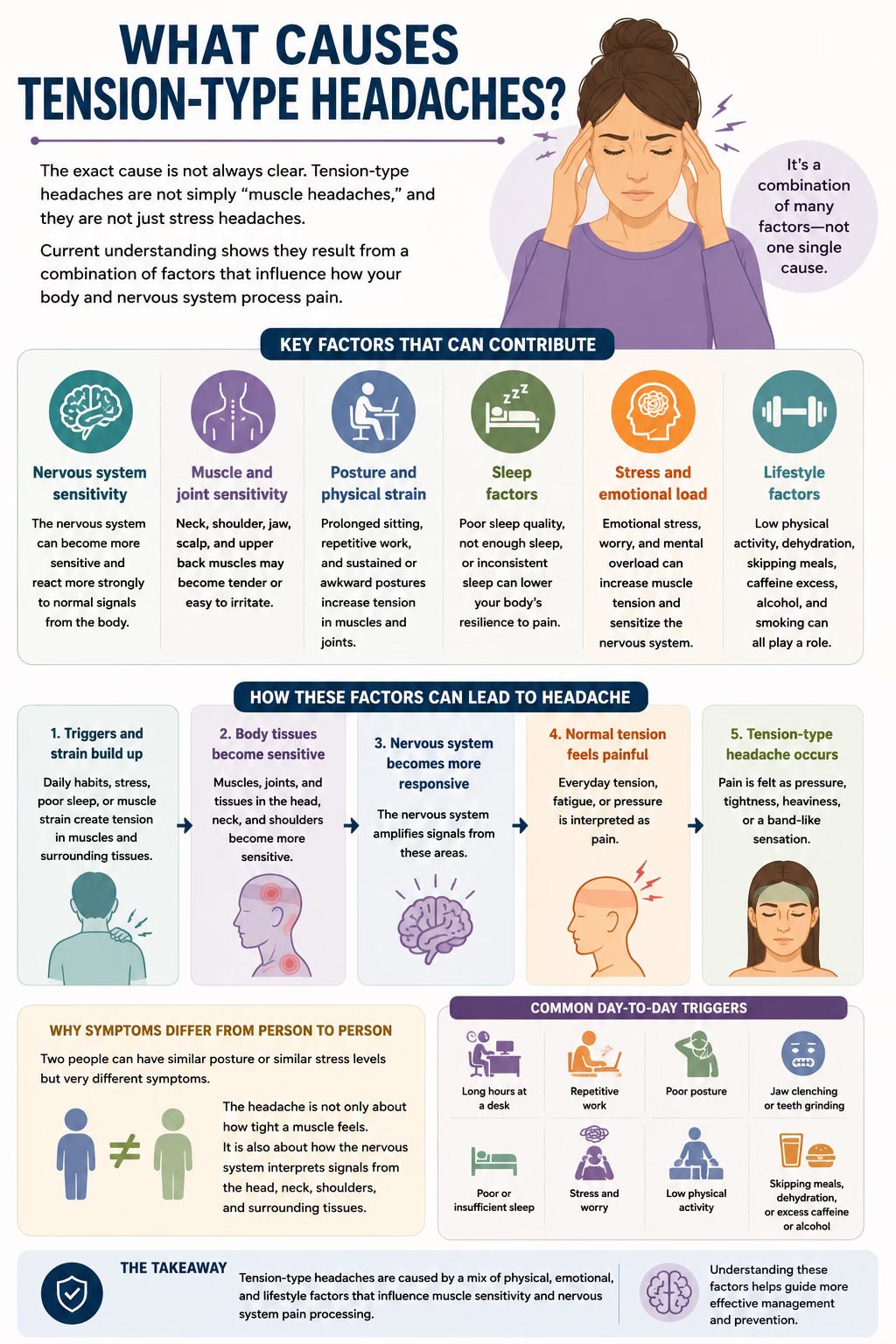
In many patients, the muscles and joints of the neck, upper back, shoulders, jaw, and scalp become sensitive. This can happen with prolonged sitting, repetitive work, poor sleep, stress, reduced movement, jaw clenching, or sustained postures. Over time, the nervous system may become more responsive to signals coming from these areas. When that happens, normal tension or fatigue can begin to feel painful.
This is one reason two people can have similar posture or similar stress levels but very different symptoms. The headache is not only about how tight a muscle feels. It is also about how the nervous system is interpreting signals from the head, neck, shoulders, and surrounding tissues.
Common Symptoms of Tension-Type Headaches
The most common symptom is a dull, pressing, tightening, or heavy sensation around the head. Patients may describe a tight hat, a band around the forehead, pressure behind the eyes, or squeezing at the temples. The pain is usually mild to moderate, but it can still be distracting and draining.
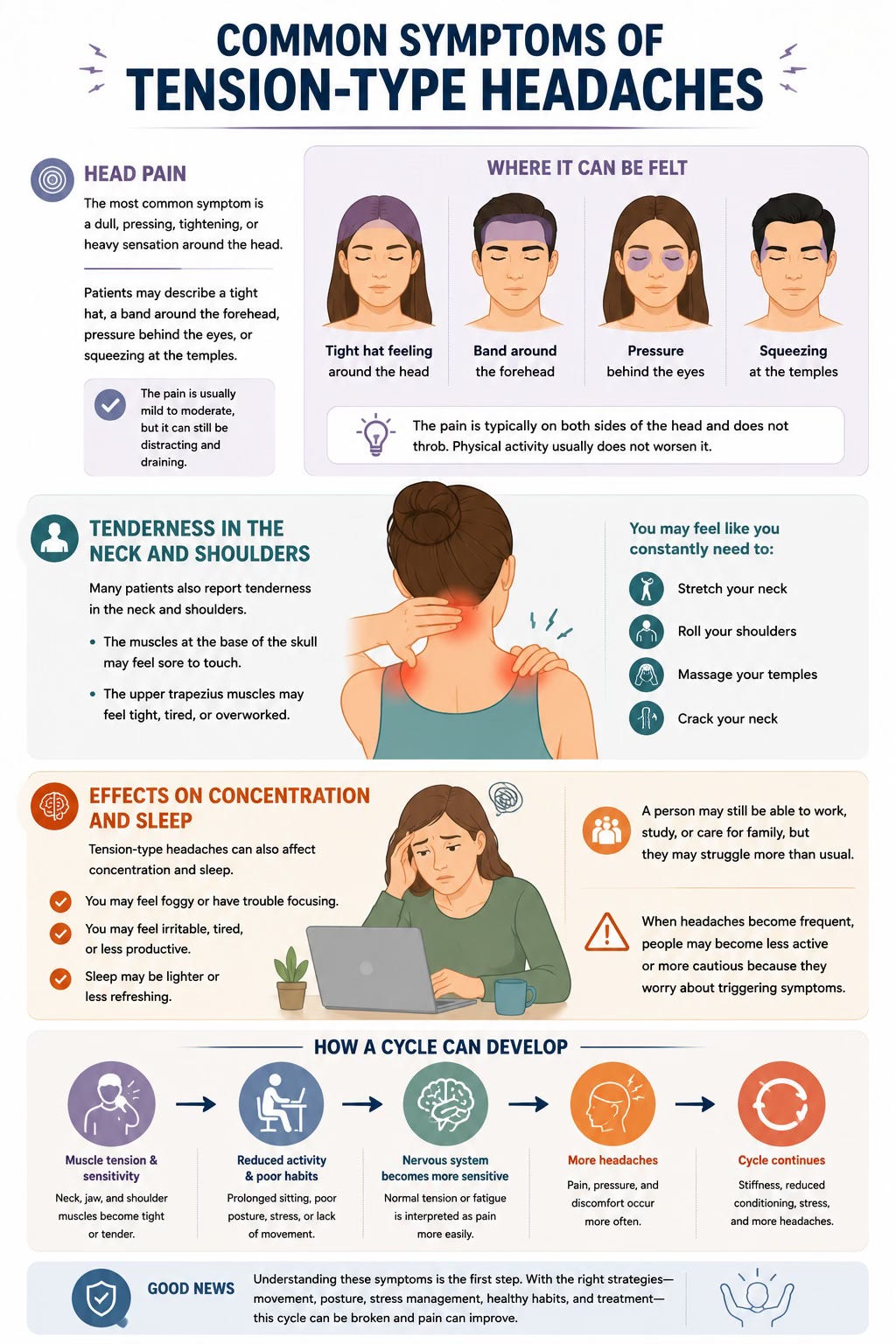
Many patients also report tenderness in the neck and shoulders. The muscles at the base of the skull may feel sore to touch. The upper trapezius muscles may feel tight, tired, or overworked. Some people feel as though they constantly need to stretch their neck, roll their shoulders, massage their temples, or crack their neck.
Tension-type headaches can also affect concentration and sleep. A person may still be able to work, study, or care for family, but they may feel foggy, irritable, tired, or less productive. When headaches become frequent, people may become less active or more cautious because they worry about triggering symptoms. Over time, this can create a cycle of stiffness, reduced conditioning, stress, and more headaches.
The Neck and Shoulder Connection
The neck and shoulders are commonly involved in tension-type headache patterns. The upper cervical spine, the base of the skull, the jaw, and the upper back all contain muscles, joints, and nerves that can contribute to head and neck discomfort. When these areas become sensitive or overloaded, symptoms can spread into the head.
Many patients describe headaches that start at the base of the skull and wrap around toward the forehead or temples. Others feel pressure across the front of the head after long periods of sitting or screen use. Some notice headaches after driving, studying, sleeping awkwardly, clenching their jaw, or looking down at a phone for long periods.
This does not mean posture is always the cause. It also does not mean every headache comes from the neck. However, when headaches occur with neck stiffness, reduced neck range of motion, shoulder tension, tenderness at the base of the skull, or symptoms that build with prolonged positions, the neck and upper back should be assessed.
What the Research Says About Therapy for Tension-Type Headaches
A 2022 systematic review and network meta-analysis published in Cephalalgia examined therapy interventions for tension-type headache. The authors searched major databases including Web of Science, Medline, Cochrane Library, and the Physiotherapy Evidence Database up to August 2021. They included randomized controlled trials involving adults diagnosed with tension-type headache according to International Headache Society criteria (Jung et al., 2022).
The review included 20 reports, and 15 were included in the network meta-analysis for headache intensity and frequency. The interventions studied included manual therapy, joint mobilization, exercise, postural correction, massage, soft tissue techniques, trigger point therapy, transcutaneous electrical nerve stimulation, relaxation, neural mobilization, dry needling, and combinations of these approaches (Jung et al., 2022).
One of the key findings was that combined approaches appeared more effective than single techniques alone. For headache intensity, transcutaneous electrical nerve stimulation combined with physiotherapy techniques was the most effective approach compared with control and usual care. The reported mean difference was −4.18 compared with control and −3.8 compared with usual care, with moderate confidence in the evidence (Jung et al., 2022).
For headache frequency, manual therapy involving joint mobilization combined with exercise and postural correction was the most effective intervention. This approach reduced headache frequency compared with control and usual care. The reported mean difference was −13.03 headache days per month compared with control and −13.95 headache days per month compared with usual care, with low to moderate confidence depending on the comparison (Jung et al., 2022).
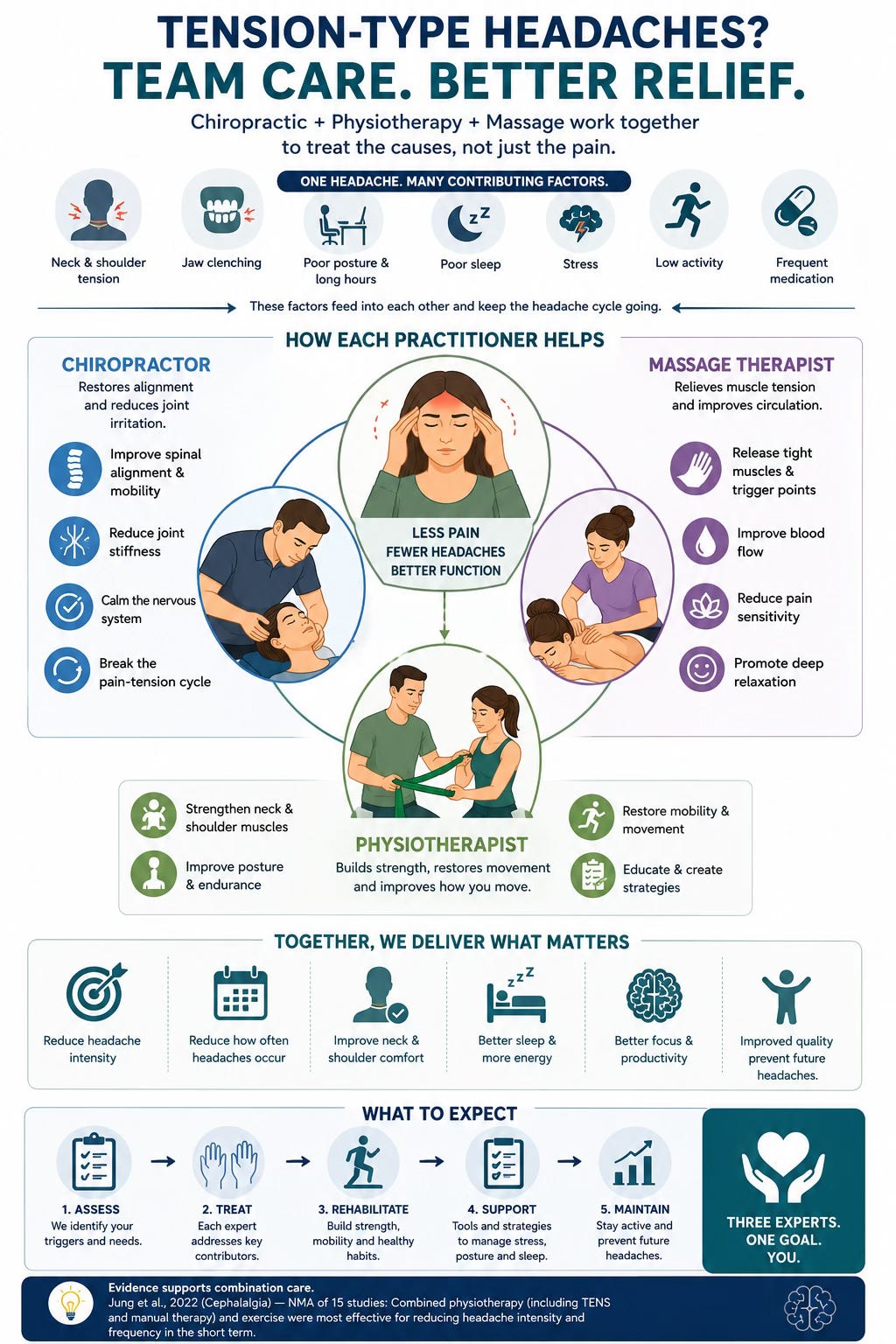
These findings are important because they support a practical clinical message: tension-type headaches often respond best to a combined care plan. Hands-on treatment may help reduce pain and sensitivity, but exercise, postural education, movement strategies, and self-management are important parts of care.
Why Combination Care Often Makes Sense
Tension-type headaches are rarely caused by one single issue. A patient may have neck stiffness, shoulder tension, jaw clenching, poor sleep, stress, long work hours, reduced activity, and frequent medication use all contributing to the same headache pattern. If care only focuses on one factor, the improvement may be incomplete or temporary.
The 2022 review found that individual therapy techniques were generally not as effective as combined approaches. For example, manual therapy alone or exercise alone did not rank as highly as manual therapy combined with exercise and postural correction for reducing headache frequency (Jung et al., 2022).
This fits what we often see clinically. A massage may help someone feel better for a short period, but if the same person returns to long hours at a desk, poor sleep, limited movement, and no strengthening plan, the headache may keep returning. Similarly, exercise can be helpful, but if the neck is very sensitive and painful, some patients may first need symptom relief and guidance before they can comfortably exercise.
A well-rounded plan may include manual therapy, soft tissue therapy, mobility work, strengthening, posture coaching, ergonomic advice, breathing strategies, sleep discussion, and education about how to respond when symptoms begin.
Medication Can Help, But It Is Not the Whole Plan
Over-the-counter medication may help occasional tension-type headaches when used safely and appropriately. However, frequent use of pain-relieving medication can sometimes contribute to medication-overuse headaches, where headaches become more frequent and harder to control.
This does not mean medication is bad. It means medication should be used thoughtfully. If someone is taking pain relievers several days per week, waking with headaches, or feeling dependent on medication to function, they should speak with a healthcare provider.
For frequent or chronic tension-type headaches, prevention becomes more important than repeatedly treating the headache after it starts. Prevention may include improving sleep, reducing prolonged static posture, strengthening the neck and upper back, managing stress, improving hydration, addressing jaw clenching, and determining whether medical management is needed.
How The Muscle and Joint Clinic Assesses Headaches
At The Muscle and Joint Clinic, assessment begins with a detailed history. We ask where the headache is located, how it feels, how often it happens, how long it lasts, what triggers it, what relieves it, and whether the pattern is changing. We also ask about nausea, light sensitivity, sound sensitivity, vision changes, dizziness, numbness, weakness, jaw pain, sleep, stress, work habits, exercise, hydration, and medication use.
This history helps us determine whether the headache pattern is most consistent with a tension-type headache, cervicogenic headache, migraine, medication-overuse headache, or another condition that may require medical referral.
The physical assessment may include checking neck range of motion, upper back mobility, shoulder mechanics, jaw tension, muscle tenderness, posture tolerance, strength, breathing patterns, and neurological screening when appropriate. We also screen for red flags that may suggest the need for medical evaluation.
The goal is not to assume every headache is muscular. The goal is to understand the headache pattern, identify contributing factors, rule out warning signs, and determine whether conservative care is appropriate.
Conservative Treatment Options
When conservative care is appropriate, treatment may include a combination of manual therapy, soft tissue therapy, mobilization, exercise, stretching, postural education, ergonomic advice, and self-management strategies. Some patients may also benefit from modalities such as heat or electrical stimulation, depending on their presentation and clinical suitability.
Manual therapy may be used to improve movement and reduce sensitivity in the neck and upper back. Soft tissue therapy may help address tenderness in the muscles around the neck, shoulders, jaw, and base of the skull. Exercise may focus on the deep neck muscles, shoulder blade control, upper back strength, postural endurance, and general conditioning.
This type of combined approach is consistent with the findings of Jung et al. (2022), who concluded that passive physiotherapy techniques combined with exercise, postural correction, and/or transcutaneous electrical nerve stimulation appeared to be among the most effective physiotherapy interventions for reducing headache intensity and frequency in the short term.
The Role of Exercise
Exercise is an important part of headache management for many patients. This does not always mean intense exercise. It may start with gentle mobility, walking, breathing exercises, and low-load strengthening.
The deep muscles of the neck help support the head during daily activity. The upper back and shoulder blade muscles help reduce unnecessary strain through the neck and shoulders. When these areas lack endurance, the body may compensate with increased tension in the upper trapezius, jaw, and base of the skull.
A good exercise plan may include gentle chin tuck variations, scapular strengthening, thoracic mobility, rows, postural endurance training, and progressive strengthening. The plan should be individualized. Too much intensity too soon may flare symptoms, while exercises that are too easy may not create meaningful change.
Posture: Important, But Often Misunderstood
Posture can contribute to tension-type headaches, but it is often oversimplified. There is no single perfect posture that prevents headaches. The body is designed to move, not to hold one position all day.
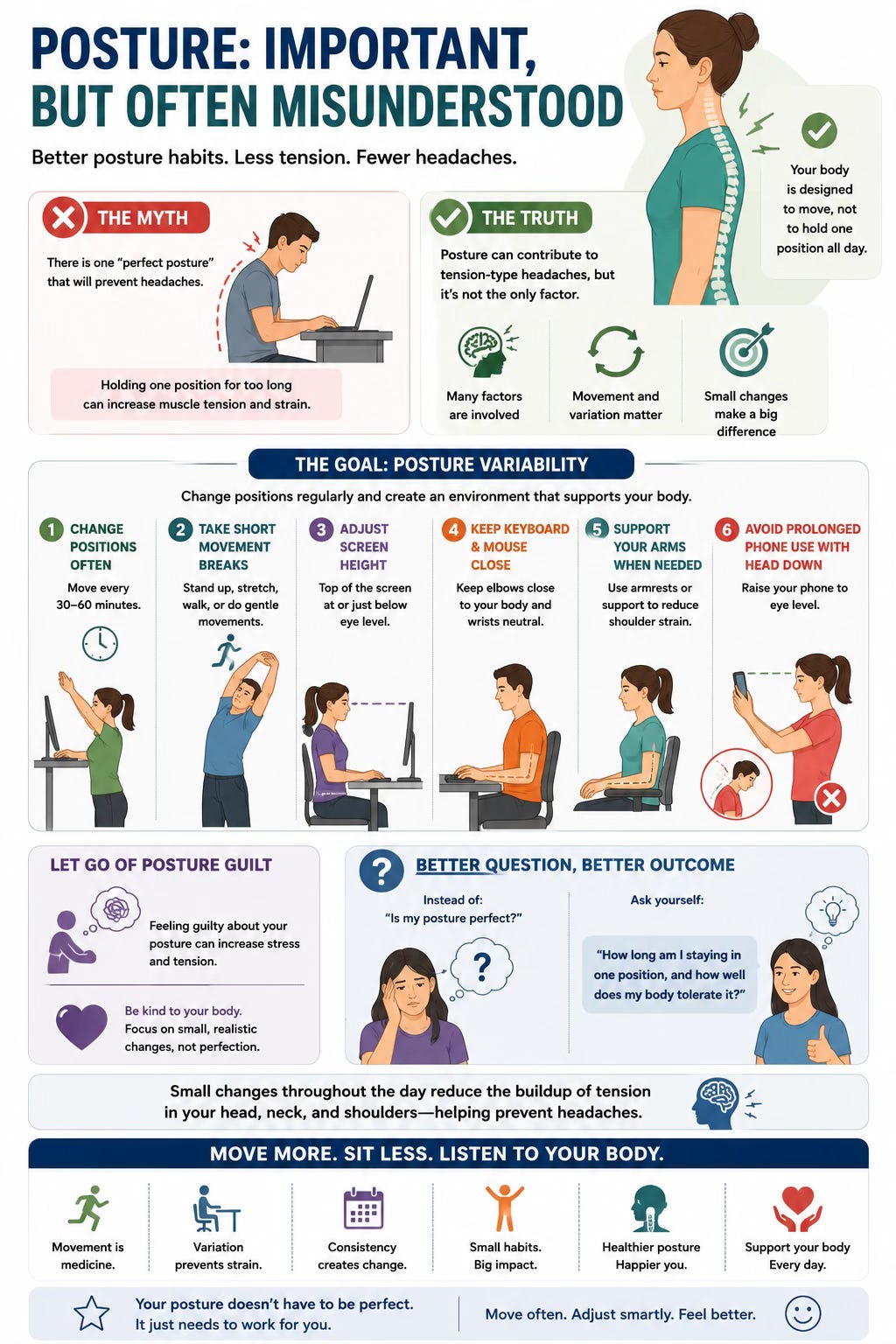
A more useful goal is posture variability. This means changing positions regularly, taking short movement breaks, adjusting screen height, keeping the keyboard and mouse close, supporting the arms when needed, and avoiding prolonged phone use with the head bent down.
Patients often feel guilty about posture, but guilt is not helpful. The better question is: how long are you staying in one position, and how well does your body tolerate that position? Small changes throughout the day can reduce the buildup of tension that often leads to headaches.
Stress, Sleep, and Jaw Tension
Stress does not mean a headache is “all in your head.” Stress creates real physical changes. During stressful periods, many people clench their jaw, raise their shoulders, breathe shallowly, sleep poorly, skip meals, increase caffeine, or reduce physical activity. These changes can all contribute to headache symptoms.
Jaw clenching is especially common. Some patients wake with temple pain, jaw soreness, or headaches near the side of the head. Others clench during work, driving, studying, or concentration without realizing it. In these cases, jaw awareness, breathing strategies, dental assessment, and neck treatment may all be relevant.
Sleep is also important. Poor sleep can increase pain sensitivity and reduce recovery. Patients with frequent headaches should pay attention to sleep quality, pillow comfort, bedtime consistency, caffeine timing, and whether they wake feeling rested.
Self-Care Strategies That May Help
For mild tension-type headaches, simple strategies may help reduce symptoms. Gentle neck and shoulder movement, walking, hydration, rest from screens, heat to the neck and shoulders, light stretching, and breathing exercises may provide relief.
Some people benefit from self-massage around the temples, jaw muscles, upper shoulders, or base of the skull. However, more pressure is not always better. Aggressive pressure can irritate sensitive tissues and worsen symptoms. Self-care should feel relieving, not aggravating.
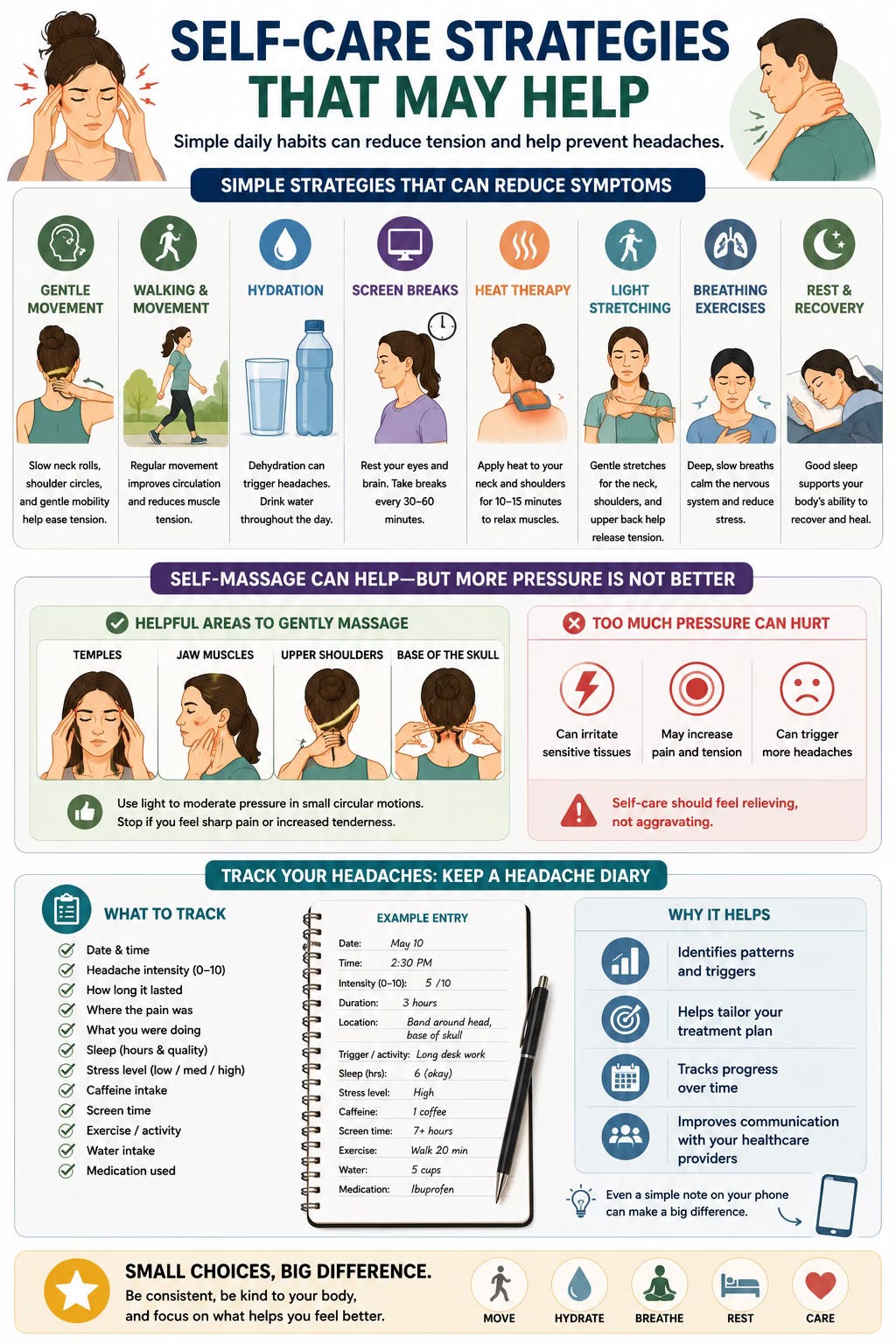
A headache diary can also be useful. Tracking headache frequency, duration, intensity, sleep, stress, caffeine, screen time, exercise, and medication use can help identify patterns. This information can make assessment and treatment more targeted.
When to Seek Medical Attention
Most tension-type headaches are not dangerous, but some headache symptoms need urgent medical assessment. Seek medical care if a headache is sudden and extremely severe, especially if it is unlike anything you have experienced before. A headache after a head injury should also be assessed.
Medical attention is also important if headache is associated with fever, neck stiffness, confusion, fainting, seizure, weakness, numbness, difficulty speaking, facial drooping, vision loss, or trouble walking. A new headache after age 50, headaches that are progressively worsening, headaches that wake you from sleep repeatedly, or headaches associated with cancer, immune suppression, or unexplained weight loss should also be evaluated.
You should also speak with a healthcare provider if headaches are increasing in frequency, if you are using pain medication frequently, or if headaches are interfering with work, school, sleep, or daily life.
What Patients Can Expect From Care
For occasional headaches, improvement may happen quickly with simple strategies. For frequent or chronic headaches, progress may take more time because the nervous system, muscles, habits, stress patterns, sleep, and medication use may all be involved.
A successful plan usually includes both short-term relief and long-term prevention. Short-term relief may come from manual therapy, soft tissue work, heat, mobility, or other symptom-relieving strategies. Long-term prevention often requires exercise, movement breaks, sleep improvements, workstation changes, stress management, and better awareness of early warning signs.
The goal is not to promise that headaches will never happen again. The goal is to reduce how often they happen, how intense they become, how long they last, and how much they interfere with life.
Final Thoughts
Tension-type headaches are common, but common does not mean unimportant. If headaches are frequent, recurring, or affecting your quality of life, they deserve proper assessment.
The research suggests that combined therapy approaches may help reduce headache intensity and frequency in the short term, especially when hands-on care is paired with exercise, postural correction, and self-management strategies (Jung et al., 2022). This supports a practical, individualized approach rather than relying on one single treatment.
At The Muscle and Joint Clinic, our goal is to help patients understand their headache pattern, rule out warning signs, identify contributing factors, and build a plan that supports long-term comfort, function, and confidence.
If you experience frequent headaches, pressure around the head, neck tightness, or headaches that build during the day, a thorough assessment can help determine whether conservative care may be appropriate for you.
References
Bendtsen, L., Evers, S., Linde, M., Mitsikostas, D. D., Sandrini, G., & Schoenen, J. (2010). EFNS guideline on the treatment of tension-type headache: Report of an EFNS task force. European Journal of Neurology, 17(11), 1318–1325. https://doi.org/10.1111/j.1468-1331.2010.03070.x
Headache Classification Committee of the International Headache Society. (2018). The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 38(1), 1–211. https://doi.org/10.1177/0333102417738202
Jung, A., Eschke, R.-C., Struss, J., Taucher, W., Luedtke, K., & collaborators. (2022). Effectiveness of physiotherapy interventions on headache intensity, frequency, duration and quality of life of patients with tension-type headache: A systematic review and network meta-analysis. Cephalalgia, 42(9), 944–965. https://doi.org/10.1177/03331024221082073
LeWine, H. E. (2026, June 16). Tension headache. Harvard Health Publishing.
Schwartz, B. S., Stewart, W. F., Simon, D., & Lipton, R. B. (1998). Epidemiology of tension-type headache. JAMA, 279(5), 381–383. https://doi.org/10.1001/jama.279.5.381