
The Digastric Muscle and TMJ Pain
The Overlooked Muscle Under the Jaw


Jaw pain is often described as “TMJ pain,” but the temporomandibular joint is only one part of the problem. The jaw is controlled by a coordinated system of joints, muscles, ligaments, nerves, teeth, posture, breathing mechanics, and neck movement. When this system becomes irritated, pain may come from the joint itself, the chewing muscles, the muscles under the jaw, or a combination of several structures.
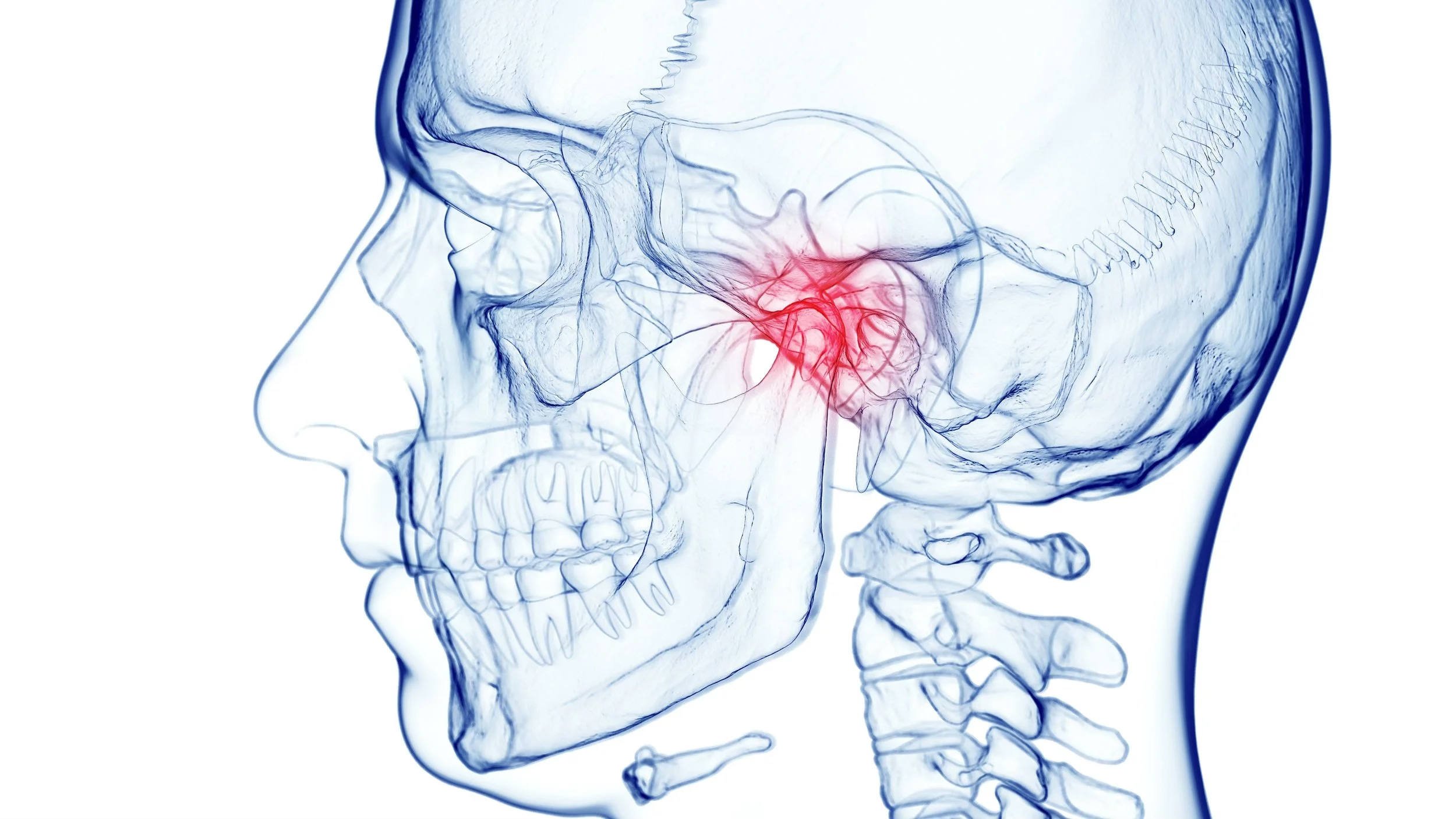
One muscle that is often overlooked in jaw pain is the digastric muscle. Although it is small, it can play an important role in temporomandibular disorders, also known as TMD. The digastric muscle helps with mouth opening, jaw depression, swallowing, and stabilization of the hyoid bone, which sits at the front of the neck. Because of its location under the jaw and near the throat, irritation in this muscle can sometimes create symptoms that feel confusing, including pain under the chin, discomfort near the throat, pain behind the jaw, ear-area pain, and even tooth-like pain.
Temporomandibular disorders are a group of conditions that can affect the jaw joint, the muscles of chewing, or both. The Diagnostic Criteria for Temporomandibular Disorders recognizes muscle-related jaw pain as an important part of TMD assessment, especially when a patient’s familiar pain is reproduced with jaw movement or muscle palpation.
What Is the Digastric Muscle?
The digastric muscle is located under the jaw and has two separate parts, known as the anterior belly and posterior belly. The anterior belly is located closer to the front of the chin and lower jaw. The posterior belly travels toward the area behind the jaw and near the mastoid region behind the ear. These two parts connect through an intermediate tendon near the hyoid bone.
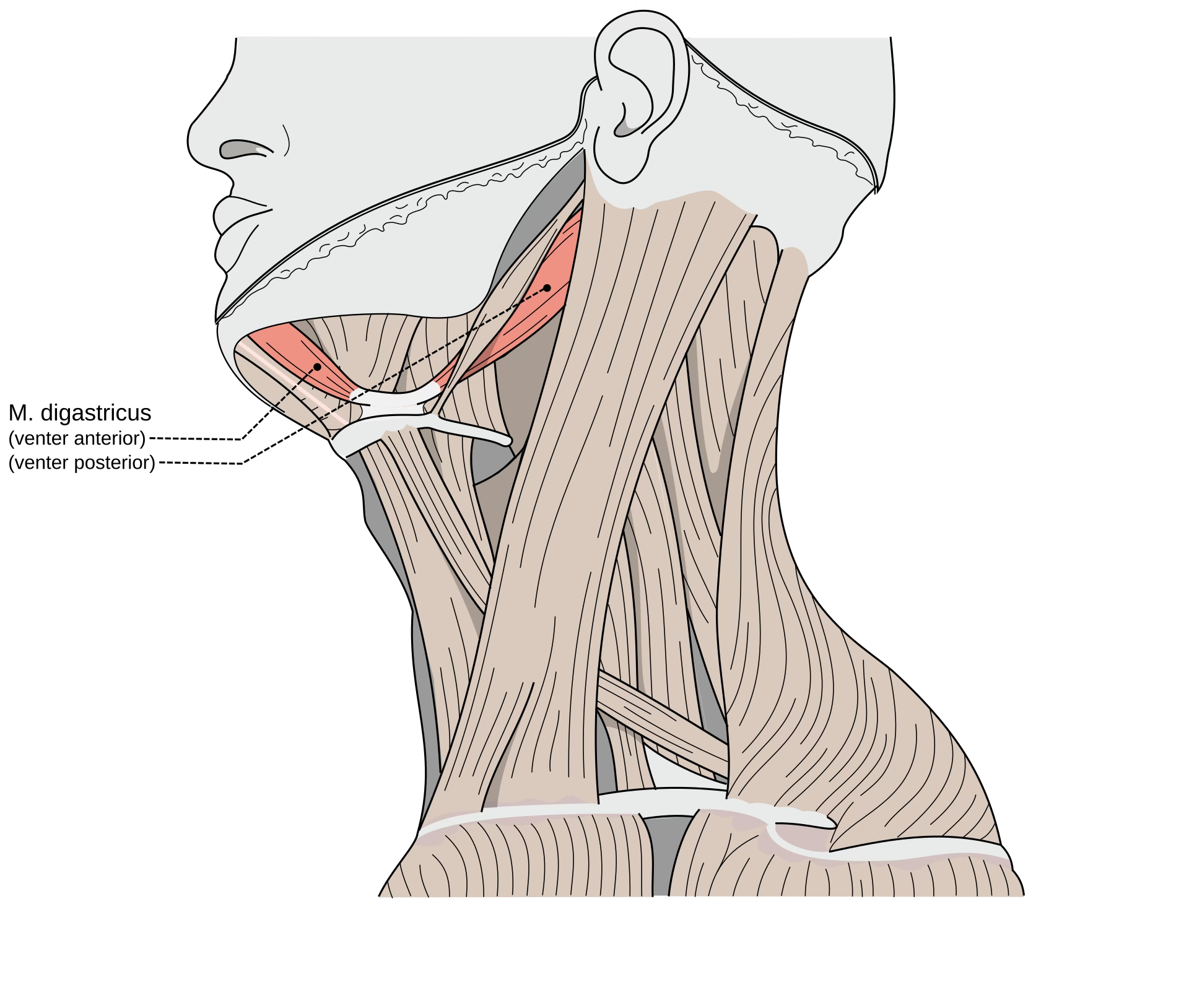
The muscle’s name comes from the fact that it has “two bellies.” Its main functions include helping open the mouth, assisting with lowering the mandible, supporting swallowing, and stabilizing the hyoid bone during movements of the tongue, jaw, and throat. Because the jaw, tongue, throat, and neck are so closely connected, increased tension in the digastric muscle can affect more than just one small area.
When the digastric muscle becomes irritated, the patient may not always feel pain directly in the muscle. Some patients feel tenderness under the chin. Others feel pain near the angle of the jaw, pressure near the throat, discomfort behind the ear, or tightness that seems to pull from the jaw into the upper neck. In some cases, the pain may even be perceived in the lower front teeth, which can make the condition feel like a dental problem rather than a muscle problem. A published case report described non-dental toothache in the mandibular anterior teeth caused by referred pain from trigger points in the anterior digastric muscle.
How the Digastric Muscle Can Contribute to TMJ Pain
The digastric muscle is involved in opening the mouth and coordinating movement between the jaw and hyoid bone. If it becomes tight, overactive, or sensitive, it can contribute to altered jaw mechanics. A patient may feel that the jaw does not open smoothly, that there is pulling under the chin, or that talking, chewing, swallowing, or yawning increases discomfort.
In many patients, digastric muscle pain does not occur alone. It may be associated with tension in the masseter, temporalis, lateral pterygoid, medial pterygoid, sternocleidomastoid, suboccipital muscles, scalenes, and upper trapezius. This is why TMJ pain often overlaps with neck pain, headaches, ear pressure, and upper shoulder tension. The jaw and neck are biomechanically linked, and changes in head posture can increase the load on muscles under the jaw.
Muscle-related TMD can be complex. Research on orofacial pain describes TMD as a condition influenced by biological, behavioural, psychological, and social factors. Jaw parafunction, clenching, grinding, stress, poor sleep, trauma, posture, and overlapping pain conditions can all contribute to the development or persistence of TMD symptoms.
Why Digastric Pain Can Feel Like Tooth, Ear, or Throat Pain
One of the most important things to understand about muscle pain is that it can refer pain to another location. A trigger point is a sensitive area within a tight band of muscle. When pressed, stretched, or irritated, it may reproduce local pain or send pain to a distant area. In the case of the anterior digastric muscle, referred pain may be felt in the lower front teeth. In the posterior portion of the muscle, symptoms may be felt closer to the throat, jaw angle, or area behind the ear.
This can create a diagnostic challenge. A patient may visit a dentist because the pain feels like a toothache. If dental causes are ruled out, the source may be muscular, neural, joint-related, or referred from another structure. This does not mean tooth pain should be ignored. Dental infection, gum disease, cracked teeth, and other dental conditions must always be properly assessed. However, when dental evaluation does not explain the symptoms, the digastric muscle and other jaw-related muscles may deserve closer attention.
This is especially relevant when pain changes with jaw movement, chewing, swallowing, neck posture, clenching, or palpation under the jaw. A careful clinical assessment can help determine whether the patient’s familiar symptoms are reproduced by testing the jaw joint, the chewing muscles, the digastric muscle, or the cervical spine.
Common Symptoms of Digastric-Related Jaw Pain
Patients with digastric muscle involvement may describe a deep ache under the jaw, tenderness below the chin, tightness near the throat, or pain around the angle of the jaw. Some may feel discomfort behind the ear or near the mastoid region. Others may notice that opening the mouth feels restricted or uncomfortable.
The symptoms may worsen with chewing, yawning, prolonged talking, singing, dental procedures, clenching, grinding, or holding the head forward for long periods. Some patients notice symptoms after stressful periods because they unknowingly clench their jaw. Others notice symptoms after long hours at a computer, where forward head posture increases strain through the jaw, neck, and throat muscles.
A patient may also describe a “lump in the throat” feeling, even when there is no true lump present. This sensation can have many causes, and medical causes should be considered when appropriate. However, muscle tension under the jaw and around the throat can sometimes contribute to this type of discomfort.
Common Causes of Digastric Muscle Irritation
Digastric muscle irritation often develops from repeated strain rather than one single event. Clenching and grinding are common contributors because they increase baseline jaw muscle activity. Even when the teeth are not grinding loudly at night, daytime clenching during work, driving, studying, exercising, or stress can keep the jaw muscles active for hours.
Forward head posture is another common factor. When the head shifts forward, the muscles at the front of the neck and under the jaw may become more active as they help support and stabilize the head, jaw, tongue, and throat. This is one reason TMJ symptoms often appear alongside neck stiffness and headaches.
Overuse habits can also irritate the digastric muscle. Chewing gum, nail biting, frequent snacking on hard foods, prolonged talking, or holding the jaw open for dental work may aggravate symptoms. Trauma, whiplash, falls, sports injuries, and direct blows to the jaw can also affect the jaw and neck system.
Stress and sleep quality matter as well. TMD is not only a mechanical condition. People under prolonged stress may clench more often, breathe differently, sleep poorly, and experience increased nervous system sensitivity. The result can be a jaw that feels tight, tired, painful, and difficult to relax.
How Digastric Muscle Pain Is Assessed
Assessment begins with a detailed history. A clinician will usually ask where the pain is located, when it started, what movements aggravate it, whether there is clicking or locking, whether dental causes have been assessed, whether headaches or neck pain are present, and whether the patient clenches or grinds.
The physical assessment may include observing jaw opening, checking for deviation or limitation, palpating jaw muscles, assessing the neck and upper shoulders, testing posture, and determining whether palpation reproduces the patient’s familiar pain. The DC/TMD framework emphasizes the importance of reproducing familiar pain during examination when assessing pain-related TMD.
For the digastric muscle specifically, the clinician may assess the area under the chin for the anterior belly and the region behind the angle of the jaw for the posterior belly. This must be done carefully because the area is sensitive and contains important structures. The goal is not to press aggressively, but to determine whether the tissue is tender, guarded, restricted, or capable of reproducing the patient’s familiar symptoms.
A good assessment should also consider the cervical spine. The jaw and neck function together, and many patients with TMJ pain also have neck stiffness, upper cervical restriction, headaches, or forward head posture. Treating only the jaw without addressing the neck may miss an important part of the problem.
Why Conservative Care Is Usually the First Step
Most muscle-related TMJ problems are initially managed with conservative, reversible care. This means treatment should usually begin with education, self-care, manual therapy, exercise, habit modification, and coordination with dental or medical providers when needed. Conservative care is especially important because not all jaw pain requires invasive treatment.
Research on manual therapy and therapeutic exercise for TMD shows that these approaches may help some patients, although study quality and treatment methods vary. This means care should be individualized rather than presented as a one-size-fits-all cure.
For many patients, improvement comes from combining several strategies. This may include reducing clenching, improving posture, calming irritated muscles, restoring jaw mobility, improving neck movement, and gradually building better control of the jaw and cervical spine.
Home Care Considerations for Digastric and TMJ Pain
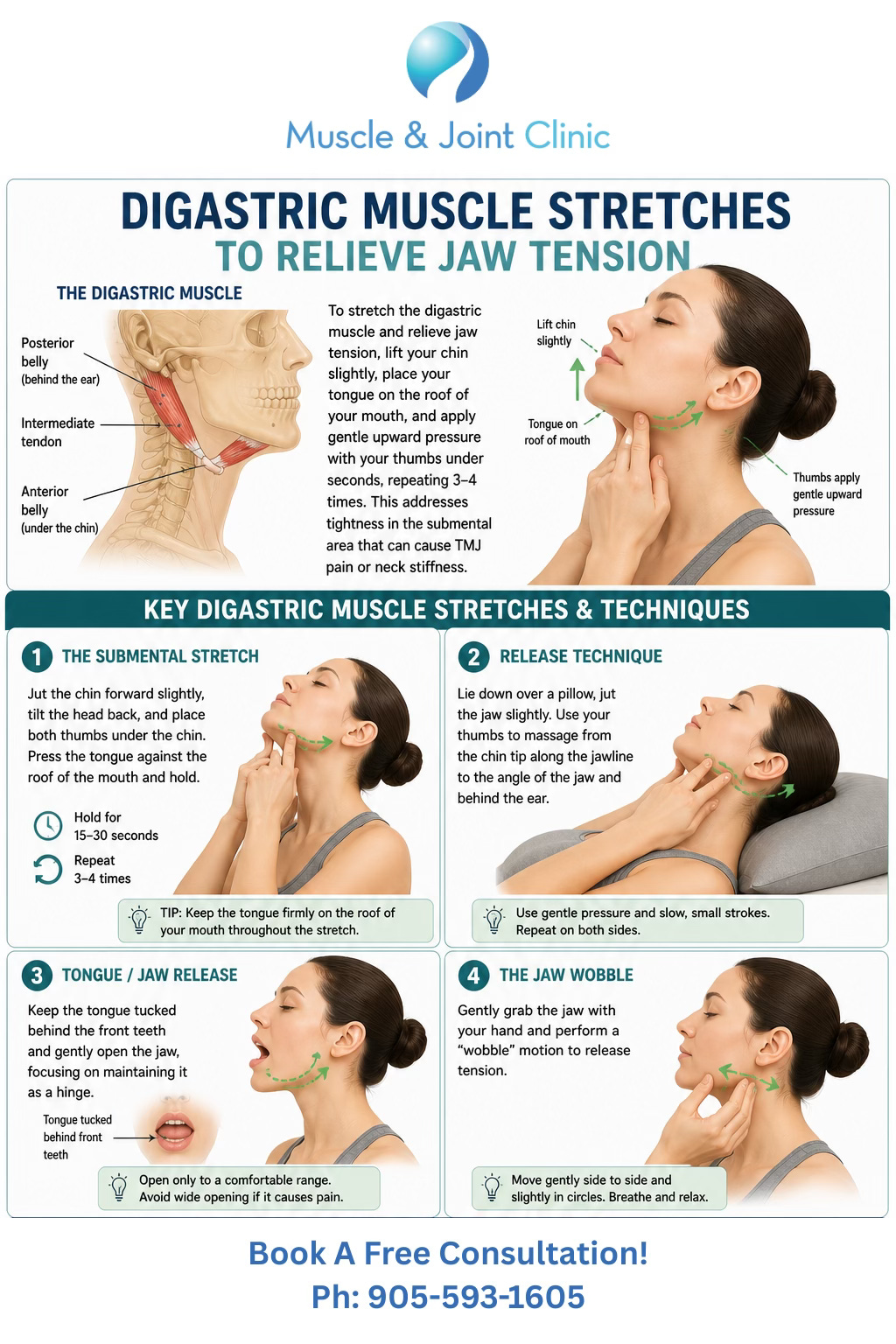
Patients with jaw muscle pain are often advised to avoid overloading the jaw while symptoms are irritated. This may include avoiding gum chewing, hard foods, wide yawning, nail biting, and unnecessary clenching. The resting position of the jaw is also important. Ideally, the lips are gently closed, the teeth are slightly apart, and the tongue rests comfortably on the roof of the mouth.
Heat may help when the area feels tight or guarded, while ice may be more appropriate when there is acute irritation or inflammation-like soreness. Gentle jaw relaxation exercises may be useful, but aggressive stretching can sometimes worsen symptoms if the tissues are highly sensitive.
Patients should also be cautious with self-massage under the jaw. This area is delicate. Light pressure may help some people, but deep or aggressive pressure near the throat, under the chin, or behind the jaw should be avoided. If symptoms are persistent, worsening, or associated with swallowing difficulty, swelling, fever, trauma, unexplained weight loss, neurological symptoms, or breathing difficulty, the patient should seek appropriate medical or dental care.
The Bigger Picture: TMJ Pain Is Often Multifactorial
It is tempting to look for one single cause of jaw pain, but TMD is often multifactorial. The digastric muscle may be one contributor, but it may not be the only one. The TMJ disc, joint capsule, masseter, temporalis, pterygoid muscles, cervical spine, posture, breathing patterns, sleep quality, stress, and dental factors may all influence symptoms.
This is why an individualized assessment matters. Two patients may both say they have “TMJ pain,” but one may primarily have joint irritation, another may have muscle-related pain, another may have neck-driven jaw symptoms, and another may have a combination of clenching, stress, poor sleep, and myofascial trigger points.
The goal of treatment is not simply to “release” one muscle. The goal is to understand the pattern of dysfunction and create a plan that reduces pain, improves movement, and helps prevent recurrence.
How The Muscle & Joint Clinic Can Help
At The Muscle & Joint Clinic in Mississauga, we take a detailed, musculoskeletal approach to TMJ-related pain. When a patient presents with jaw pain, pain under the chin, throat-area tightness, tooth-like discomfort without a clear dental cause, headaches, or neck tension, we assess the jaw as part of a larger movement system. This includes the TMJ, chewing muscles, digastric muscle, neck, shoulders, posture, breathing mechanics, and daily habits such as clenching, grinding, computer posture, and sleep position.
Our first step is to understand the patient’s story. We look at when the symptoms started, what makes them better or worse, whether the pain is related to chewing or opening the mouth, whether there are headaches or neck symptoms, whether dental causes have been ruled out, and whether the patient has habits such as jaw clenching, gum chewing, nail biting, or prolonged forward head posture. This helps us determine whether the digastric muscle is likely contributing to the pain or whether another structure may be the primary driver.
Manual muscle release techniques may be used to address excessive tension in the digastric muscle and surrounding jaw and neck muscles. These techniques involve careful, targeted pressure combined with controlled movement. The goal is to reduce muscle guarding, improve tissue mobility, and help the jaw move more comfortably. We may work not only under the jaw, but also through related areas such as the masseter, temporalis, sternocleidomastoid, scalenes, suboccipitals, and upper trapezius, depending on the patient’s presentation.
We may also use IASTM, which stands for Instrument-Assisted Soft Tissue Mobilization. This technique uses a specialized tool to gently assess and treat soft tissue restrictions. In TMJ-related cases, IASTM is usually applied to related neck, shoulder, and jaw-supporting tissues rather than aggressively over sensitive throat structures. The purpose is to improve soft tissue glide, reduce tone, improve movement quality, and help the patient tolerate exercise and posture correction more comfortably.
Laser therapy may be used as part of the treatment plan when the goal is to reduce pain sensitivity and support tissue recovery. Laser therapy, also called photobiomodulation or low-level laser therapy, uses light energy applied to targeted tissues. For TMJ-related muscle pain, it may be used around irritated soft tissues or related jaw and neck regions. It is non-invasive and typically comfortable. We use it as an adjunct to care, meaning it supports the overall treatment plan rather than replacing assessment, manual therapy, exercise, and habit correction.
Therapeutic ultrasound may also be considered when soft tissues are tender, guarded, or irritated. Ultrasound uses sound wave energy to create a therapeutic effect in soft tissues. In a clinical setting, it may be used to support circulation, reduce muscle guarding, and prepare tissues for manual therapy or movement. Like laser therapy, ultrasound is not used as a stand-alone solution; it works best when combined with hands-on treatment and active rehabilitation.
IFC, or Interferential Current Therapy, may be used when pain is more irritable or when muscle guarding makes movement difficult. IFC uses gentle electrical stimulation to help calm pain and reduce protective muscle tension. Patients often describe the sensation as a comfortable tingling. In TMJ-related cases, IFC may be applied to the neck, upper shoulder, or related muscular regions depending on the assessment. The goal is to decrease pain enough so the patient can move better and participate more effectively in rehabilitation.
A major part of care is education. Many patients do not realize how often they clench during the day. We help patients recognize resting jaw posture, reduce unnecessary jaw tension, and understand how posture, stress, sleep, and work habits may be contributing to their symptoms. Simple changes such as keeping the teeth slightly apart at rest, avoiding gum chewing, modifying workstation posture, taking jaw relaxation breaks, and reducing prolonged forward head positions can make a meaningful difference.
We also prescribe individualized exercises. These may include controlled jaw opening, tongue-position drills, gentle cervical mobility, chin tuck progressions, breathing exercises, scapular control, and postural strengthening. The goal is to improve coordination between the jaw and neck rather than simply stretching the jaw aggressively. Exercises are selected based on the patient’s pain level, mobility, sensitivity, and functional goals.
When appropriate, we also coordinate care with dentists, physicians, or other providers. If symptoms suggest dental disease, infection, significant joint pathology, neurological involvement, or another medical issue, referral is important. TMJ care is often most effective when the right providers are involved at the right time.
For patients dealing with digastric-related TMJ pain, our clinic’s approach is focused on finding the underlying contributors, calming irritated tissues, restoring comfortable movement, and helping the patient understand what to do outside the treatment room. The digastric muscle may be small, but when it is part of the problem, addressing it properly can make a significant difference in jaw comfort, neck tension, and daily function.
Book an Appointment
If you are experiencing jaw pain, TMJ discomfort, tightness under the chin, pain near the throat, headaches, ear-area discomfort, or tooth-like pain that has not been clearly explained, The Muscle & Joint Clinic in Mississauga can help assess whether the jaw muscles, neck, posture, or clenching habits may be contributing.
Book an appointment online today and let our team help you move, chew, speak, and function more comfortably.
References
Armijo-Olivo, S., Pitance, L., Singh, V., Neto, F., Thie, N., & Michelotti, A. (2016). Effectiveness of manual therapy and therapeutic exercise for temporomandibular disorders: Systematic review and meta-analysis. Physical Therapy, 96(1), 9–25.
Kalladka, M., Thondebhavi, M., Ananthan, S., Kalladka, G., & Khan, J. (2020). Myofascial pain with referral from the anterior digastric muscle mimicking a toothache in the mandibular anterior teeth: A case report. Quintessence International, 51(1), 56–62.
Kalladka, M., Ananthan, S., Viswanath, A., Thomas, D., Young, A., Singh, S., & Khan, J. (2024). Musculoskeletal disorders and orofacial pain: A narrative review. Frontiers of Oral and Maxillofacial Medicine, 6, 17.
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., … Dworkin, S. F. (2014). Diagnostic Criteria for Temporomandibular Disorders for clinical and research applications. Journal of Oral & Facial Pain and Headache, 28(1), 6–27.