
Understanding Lower Cross Syndrome: Causes, Effects, and Evidence-Based Treatment


Lower Cross Syndrome (LCS) is a common but often overlooked musculoskeletal condition that affects posture, movement, and overall function. It is characterized by a predictable pattern of muscle imbalance, where certain muscles become tight and overactive while others become weak and inhibited. This imbalance typically develops due to prolonged sitting, repetitive movements, or inactivity, all of which are increasingly common in modern lifestyles (Ghaffari et al., 2026; Janda, 1987). Over time, these patterns can lead to postural changes such as anterior pelvic tilt and increased curvature of the lower back, known as lumbar hyperlordosis.
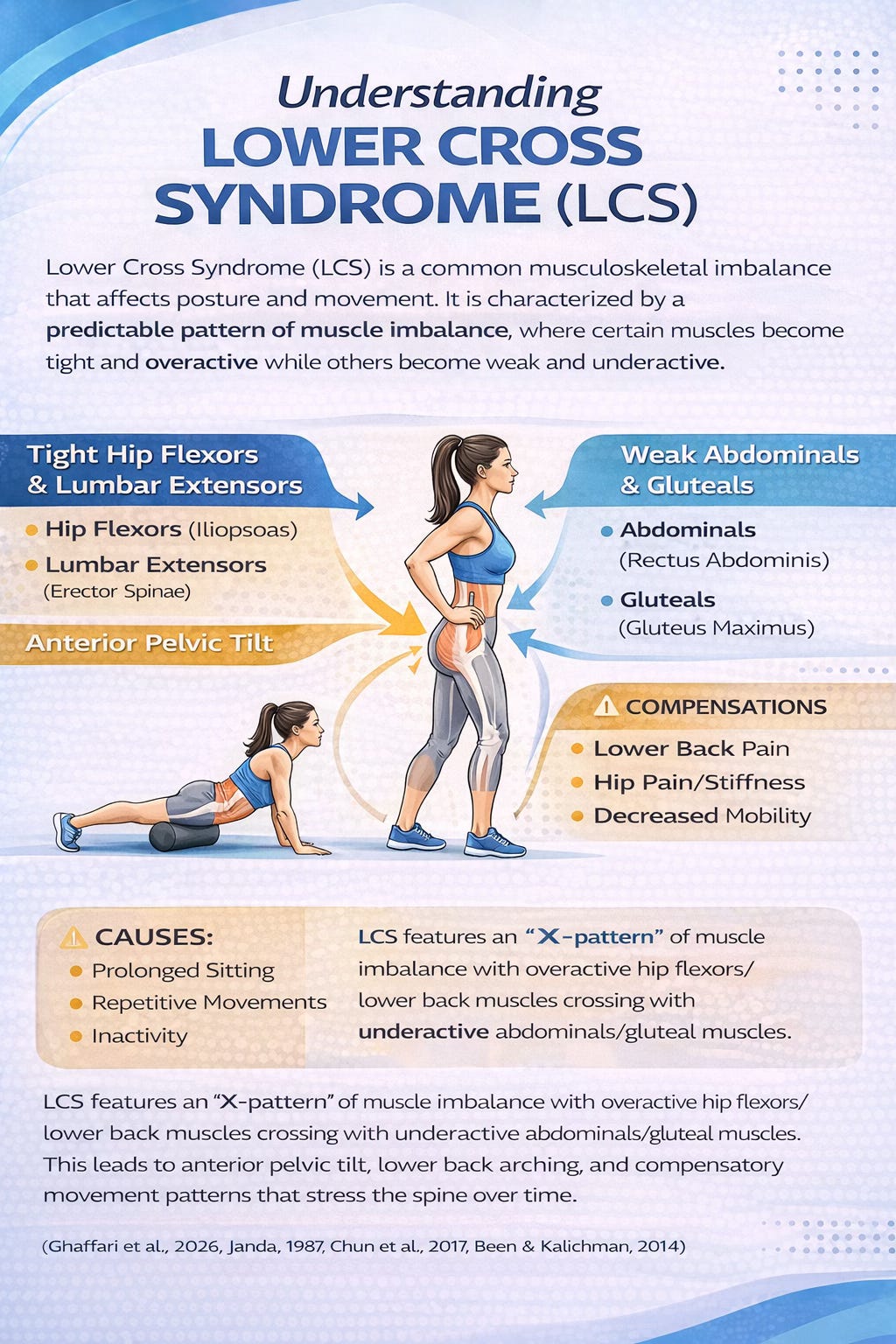
At the core of LCS is a disruption in the balance between the anterior and posterior muscle chains. The hip flexors (such as the iliopsoas) and lumbar extensors (such as the erector spinae) tend to become tight and dominant, while the abdominal muscles and gluteal muscles become weak and underactive (Ghaffari et al., 2026; Key, 2010). This creates a “crossed” pattern of dysfunction across the pelvis. As a result, the pelvis tilts forward, the lower back arches excessively, and the body compensates by altering movement patterns. These compensations are not just cosmetic, they can lead to pain, reduced efficiency in movement, and increased stress on the spine and surrounding structures (Chun et al., 2017; Been & Kalichman, 2014).
One of the most important functional consequences of LCS is altered muscle activation, particularly in the gluteus maximus. Research has shown that individuals with LCS often experience delayed activation of this key stabilizing muscle, sometimes by as much as 370 milliseconds during movement (Ghaffari et al., 2026). This delay forces other muscles, such as the hamstrings, to compensate, which can further reinforce dysfunctional movement patterns (Lehman et al., 2004). Over time, this inefficient neuromuscular coordination can impact walking, exercise performance, and even daily activities.
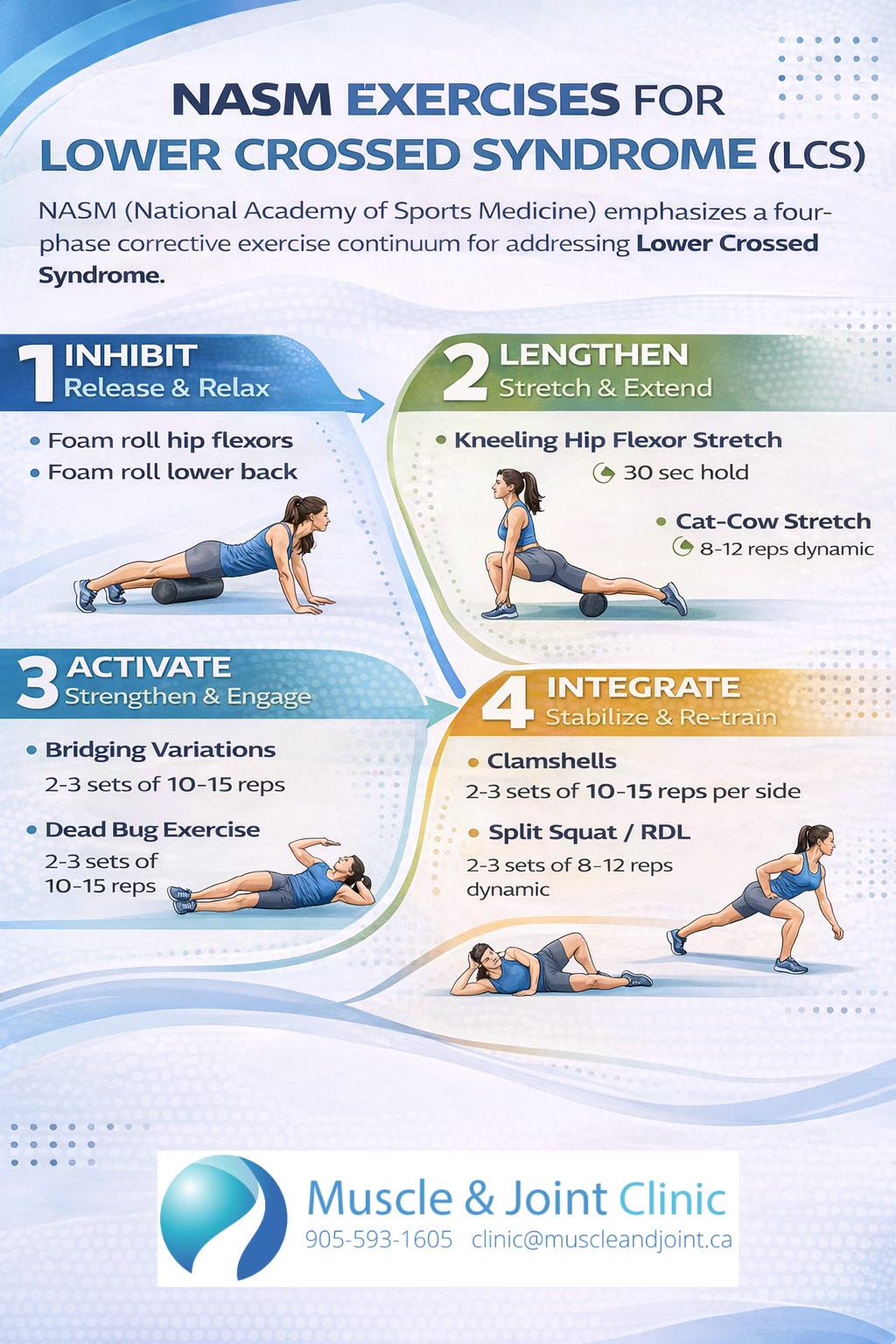
Recent research has focused on how to effectively correct these imbalances, with growing evidence supporting structured corrective exercise programs. One of the most widely studied approaches is the NASM (National Academy of Sports Medicine) corrective exercise model, which follows a systematic four-phase process: inhibition, lengthening, activation, and integration (Clark & Lucett, 2010). This approach is designed to first reduce tension in overactive muscles, then restore proper length, activate weakened muscles, and finally retrain coordinated movement patterns.
A 2026 randomized controlled trial by Ghaffari and colleagues provides strong evidence supporting this approach. In the study, women with LCS who completed an eight-week NASM corrective exercise program showed significant improvements in lumbar lordosis angle and gluteus maximus activation compared to a control group (Ghaffari et al., 2026). Specifically, participants experienced a measurable reduction in excessive spinal curvature and improved muscle function, particularly in the glutes, which play a critical role in stabilizing the pelvis and supporting efficient movement. These findings are consistent with earlier studies demonstrating that targeted corrective exercises can reduce postural abnormalities and improve neuromuscular control (Okhli et al., 2019; Ghadirian Marnani et al., 2024).
Interestingly, while improvements were seen in several muscle groups, the most significant changes occurred in the primary targets of the program, lumbar alignment and gluteal activation. This suggests that effective treatment of LCS requires a focused and structured approach rather than generalized exercise. Strengthening the glutes and core while reducing tension in the hip flexors and lower back appears to be key in restoring proper biomechanics (Ghaffari et al., 2026). These changes not only improve posture but may also reduce strain on the spine and decrease the risk of chronic low back pain (Cho et al., 2015).
From a clinical perspective, this research reinforces an important message: LCS is not simply a posture issue, it is a functional problem involving coordination, muscle balance, and movement patterns. Addressing it requires more than stretching or strengthening alone. Instead, a comprehensive strategy that targets both neuromuscular control and structural alignment is essential. As more evidence emerges, structured corrective exercise programs like NASM are becoming a cornerstone in the management of this condition.
Lower Cross Syndrome is a widespread condition driven by modern lifestyle habits and characterized by predictable patterns of muscle imbalance. These imbalances can lead to postural changes, inefficient movement, and increased risk of pain and dysfunction. However, research shows that targeted, evidence-based corrective exercise programs can effectively restore balance, improve muscle activation, and reduce abnormal spinal curvature. For individuals experiencing lower back discomfort, poor posture, or movement limitations, identifying and addressing LCS may be a critical step toward long-term recovery and improved function.
References (APA)
Been, E., & Kalichman, L. (2014). Lumbar lordosis. The Spine Journal, 14(1), 87–97. https://doi.org/10.1016/j.spinee.2013.07.464
Cho, I. Y., Park, S. Y., Park, J. H., Kim, T. K., Jung, T. W., & Lee, H. M. (2015). The effect of standing and different sitting positions on lumbar lordosis. Asian Spine Journal, 9(5), 762–769. https://doi.org/10.4184/asj.2015.9.5.762
Chun, S. W., Lim, C. Y., Kim, K., Hwang, J., & Chung, S. G. (2017). The relationships between low back pain and lumbar lordosis. The Spine Journal, 17(8), 1180–1191. https://doi.org/10.1016/j.spinee.2017.04.034
Clark, M., & Lucett, S. (2010). NASM essentials of corrective exercise training. Lippincott Williams & Wilkins.
Ghaffari, S., Hosseini, S. M., & Gheitasi, M. (2026). The effect of NASM-based corrective exercises on lumbar lordosis angle and selected muscle activity in women with lower cross syndrome: A randomized clinical trial. PLOS ONE, 21(3), e0337804. https://doi.org/10.1371/journal.pone.0337804
Ghadirian Marnani, L., Fatahi, H., Esmaeilian, M., & Rostami, S. (2024). The effect of eight weeks of NASM training on pelvic tilt and lordosis in individuals with LCS. Journal of Rehabilitation Sciences Research.
Janda, V. (1987). Muscles and motor control in low back pain. In Physical therapy of the low back.
Key, J. (2010). The pelvic crossed syndromes. Journal of Bodywork and Movement Therapies, 14(3), 299–301.
Lehman, G. J., Lennon, D., Tresidder, B., Rayfield, B., & Poschar, M. (2004). Muscle recruitment patterns during the prone leg extension. BMC Musculoskeletal Disorders, 5, 3.
Okhli, H., Hojjati, H., & Akhoundzadeh, G. (2019). Comparing NASM and Pilates exercises on lordosis correction. International Journal of School Health, 6(4).