
Understanding the Sartorius Muscle
The Overlooked Cause of Inner Knee Pain


Earlier today, a patient came into the clinic with persistent knee pain that had been bothering him for weeks. He assumed the problem was inside the knee joint. This is a very common assumption. When pain is felt at the knee, most people think the knee must be the problem.
But after a detailed assessment, the real cause turned out to be something most people have never heard of: sartorius tendinopathy.
This condition is surprisingly common, frequently misunderstood, and often misdiagnosed. The good news is that it responds very well to the right type of treatment, especially when the full movement chain is addressed.
Let’s take a deeper look.
Understanding the Sartorius Muscle
e
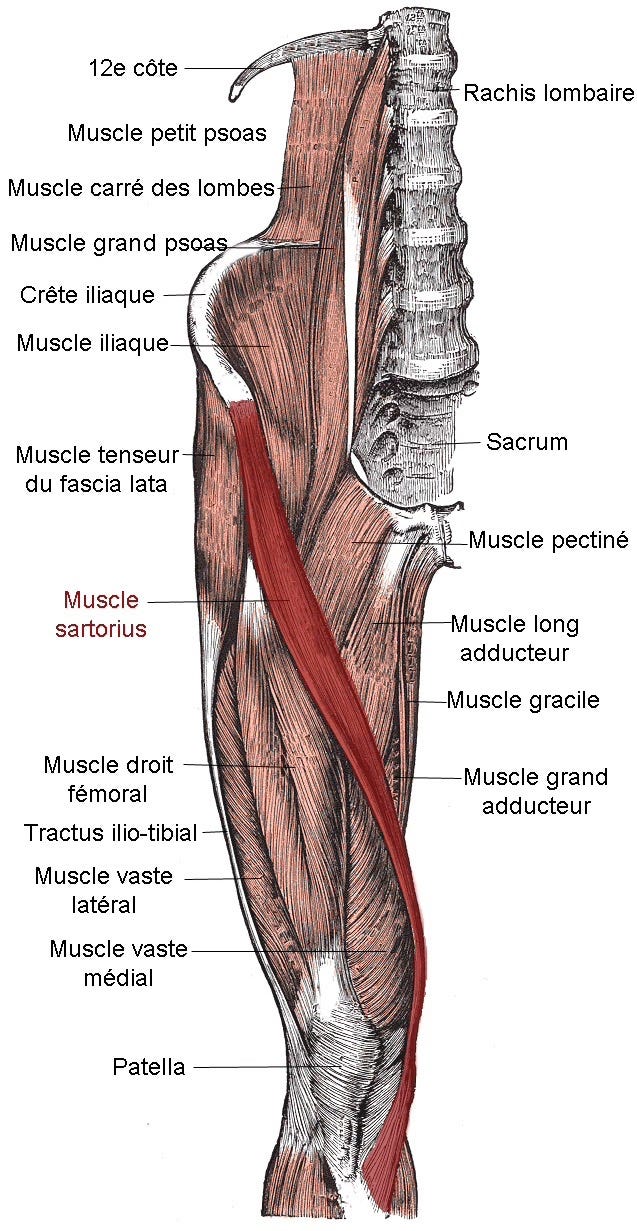
The sartorius is the longest muscle in the human body. It begins at the front of the pelvis and travels diagonally across the thigh before attaching to the inside of the upper shin bone near the knee. At the knee, it joins two other tendons to form a structure called the pes anserinus, which helps stabilize the inner side of the knee.
Because the sartorius crosses both the hip and the knee, it plays a role in several everyday movements. It helps lift your leg, rotate your hip outward, move your leg away from your body, bend your knee, and stabilize the knee while you walk (Cardoso et al., 2019).
In simple terms, this muscle is active almost all day. Every time you walk, climb stairs, get into a car, sit cross-legged, or perform lunges or squats, the sartorius is working in the background to control your leg and keep your knee stable. Because it connects the pelvis, hip, and knee, problems at the hip or pelvis can easily increase strain on the tendon where it attaches near the knee.
What Is Tendinopathy? (And Why It’s Not Just “Inflammation”)
For many years, tendon pain was described as tendonitis, suggesting inflammation was the main problem. Modern research has changed this understanding.
Studies examining tendon tissue under a microscope show that chronic tendon pain is usually caused by degeneration rather than inflammation (Kaux et al., 2011). Instead of inflamed tissue, researchers typically see disorganized collagen fibers, increased fluid-like ground substance, and the growth of small new blood vessels in the tendon (Crowe et al., 2023).
Today, experts describe tendinopathy as a failed healing response caused by repeated overload. The tendon is not inflamed, it is struggling to adapt to the demands being placed on it (Crowe et al., 2023).
This explains why rest, ice, or anti-inflammatory medications may provide temporary relief but rarely solve the problem long-term. These strategies reduce pain but do not rebuild the tendon’s strength or capacity.
Why Sartorius Tendinopathy Develops
Tendons are designed to adapt to stress. When we gradually increase activity, tendons become stronger and more resilient. However, problems occur when activity increases too quickly.
Research shows that sudden increases in physical load are one of the strongest predictors of tendinopathy (Cardoso et al., 2019). Common triggers include:
• Increasing walking or running distance
• Starting a new gym program
• Doing more lunges or squats
• Hill or stair climbing
• Returning to activity after time off
• Weak hip or glute muscles
• Changes in walking or running mechanics
When the hip stabilizing muscles are weak or not working efficiently, the sartorius tendon must work harder to control the leg during walking. Over time, the tendon becomes overloaded and painful.
Why It Is Often Mistaken for a Knee Problem
People with sartorius tendinopathy usually feel pain on the inside of the knee. Because of this, many assume the knee joint itself is damaged.
Common symptoms include:
• Pain along the inner knee
• Tenderness when pressing the area
• Pain climbing stairs
• Discomfort getting in and out of a car
• Pain when bending the knee against resistance
However, research shows that weakness in the hip muscles can significantly increase stress on the inner knee (Cardoso et al., 2019). This means the knee pain is often a symptom of a problem higher up the chain.
The knee hurts, but the real driver is frequently the hip and pelvis.
The Evidence for Progressive Loading
One of the most important discoveries in tendon research is that exercise is the most effective treatment.
Systematic reviews consistently show that progressive strengthening programs, especially eccentric and heavy slow resistance training, are the most reliable treatments for tendinopathy (Irby et al., 2020; Cooper et al., 2023).
These exercises help by:
• Improving tendon stiffness
• Increasing load tolerance
• Encouraging collagen repair
• Reducing pain over time
Tendons heal slowly, so progress must be gradual. Most rehabilitation programs take several months to fully restore tendon health.
How Chiropractic Care Fits Into Evidence-Based Management
Sartorius tendinopathy rarely occurs in isolation. It is usually part of a larger movement problem involving the pelvis, hip, and lower limb.
Restoring Joint Mechanics
Restricted movement in the pelvis, lower back, hip, or ankle can change how forces travel through the leg. Chiropractic adjustments help restore joint motion and improve movement patterns (Pfefer et al., 2008). When joints move properly, stress on the tendon decreases.
Soft Tissue Treatment
Manual therapy can reduce tension in surrounding muscles such as the hip flexors, adductors, and quadriceps. While evidence for friction massage alone is limited, it can be helpful when combined with exercise therapy (Andres & Murrell, 2008).
Progressive Rehabilitation
Rehabilitation typically progresses through stages:
Isometric exercises to reduce pain
Controlled strengthening
Heavy resistance training
Return to full activity
Most patients recover within 3–6 months when loading is progressed appropriately (Wilson & Best, 2005).
Adjunct Therapies
Shockwave and laser therapy may improve outcomes when combined with exercise (Irby et al., 2020; Maffulli et al., 2010). However, exercise remains the most important treatment.
Why Painkillers and Injections Aren’t the Long-Term Fix
NSAIDs and corticosteroid injections can reduce pain temporarily, but they do not improve long-term tendon healing and may even interfere with collagen repair when overused (Kane et al., 2019).
True recovery requires rebuilding tendon strength.
Clinical Takeaway
Sartorius tendinopathy highlights an important principle: knee pain is often a whole-body problem.
Successful recovery requires:
• Accurate diagnosis
• Assessment of movement mechanics
• Progressive strengthening
• Restoring hip and pelvic stability
When these elements are combined, most patients recover without surgery.
References
Andres, B. M., & Murrell, G. A. C. (2008). Treatment of tendinopathy: What works, what does not, and what is on the horizon. Clinical Orthopaedics and Related Research, 466(7), 1539–1554.
Cardoso, T. B., Pizzari, T., Kinsella, R., Hope, D., & Cook, J. (2019). Current trends in tendinopathy management. Best Practice & Research Clinical Rheumatology, 33(1), 122–140.
Cooper, K., Alexander, L., Brandie, D., et al. (2023). Exercise therapy for tendinopathy. Health Technology Assessment, 27(12).
Crowe, L. A. N., Akbar, M., & de Vos, R. J. (2023). Pathways driving tendinopathy and enthesitis. The Lancet Rheumatology, 5(3), e151–e162.
Irby, A., Gutierrez, J., Chamberlin, C., Thomas, S. J., & Rosen, A. B. (2020). Clinical management of tendinopathy. Scandinavian Journal of Medicine & Science in Sports, 30(10), 1815–1838.
Kane, S. F., Olewinski, L. H., & Tamminga, K. S. (2019). Management of chronic tendon injuries. American Family Physician, 100(3), 147–157.
Kaux, J. F., Forthomme, B., Goff, C. L., Crielaard, J. M., & Croisier, J. L. (2011). Current opinions on tendinopathy. Journal of Sports Science & Medicine, 10(2), 238–253.
Maffulli, N., Longo, U. G., & Denaro, V. (2010). Novel approaches for the management of tendinopathy. The Journal of Bone and Joint Surgery, 92(15), 2604–2613.
Pfefer, M. T., Cooper, S. R., & Uhl, N. L. (2008). Chiropractic management of tendinopathy. Journal of Manipulative and Physiological Therapeutics, 31(6), 464–473.
Wilson, J. J., & Best, T. M. (2005). Common overuse tendon problems. American Family Physician, 72(5), 811–818.