
What You Need To Know About Anterior Head Carriage
Why Forward Head Posture Matters More Than Most People Realize

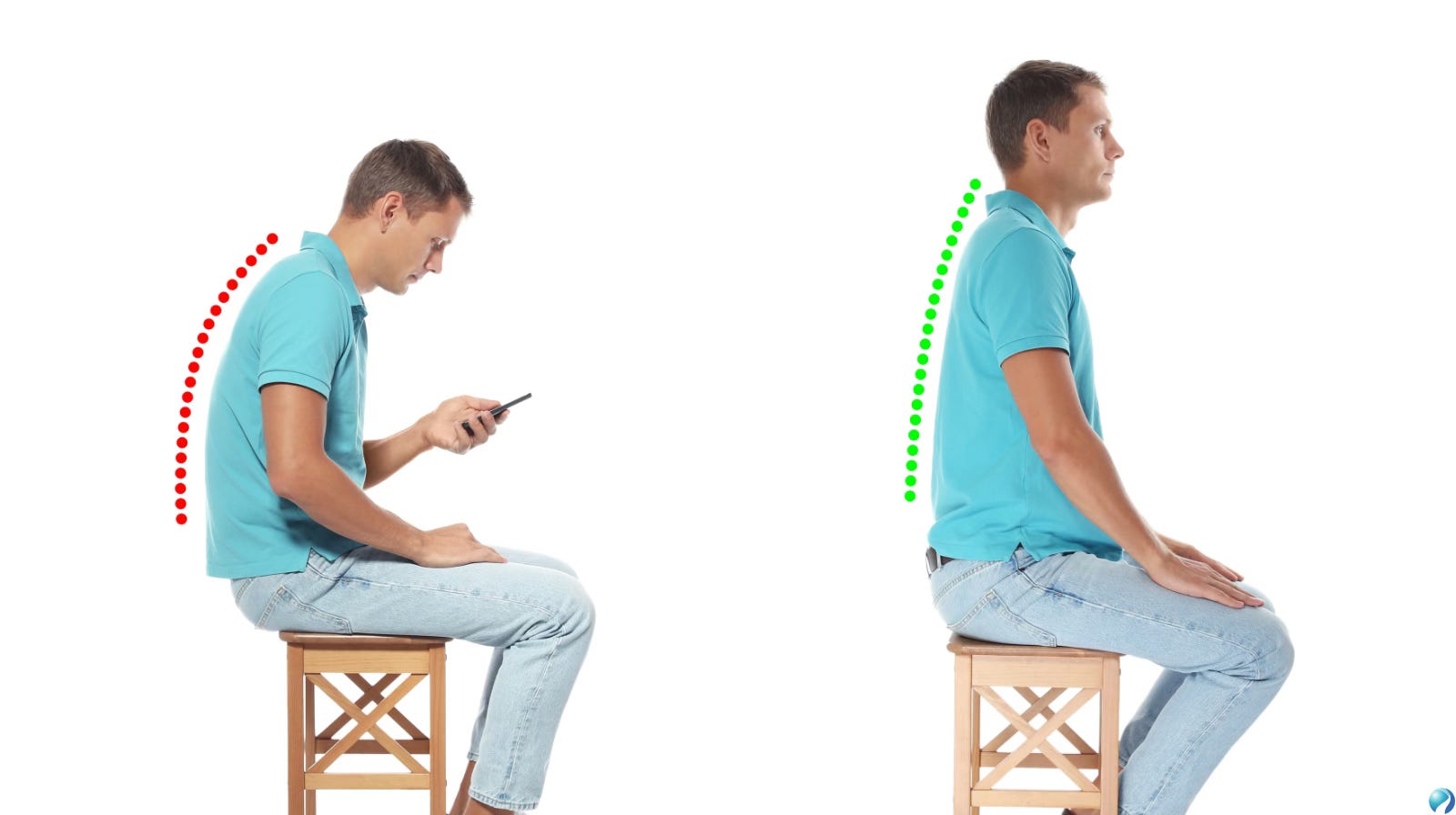
Most people think of posture as something cosmetic. It is often treated like a matter of appearance, standing tall, pulling the shoulders back, and trying not to slouch. But posture is much more than that. It is a reflection of how your body is managing gravity, movement, and load every single day. One of the most common postural changes seen today is forward head posture, also called anterior head carriage. This pattern happens when the head drifts in front of the shoulders instead of sitting in a balanced position over the spine. It may seem small when looking in the mirror, but over time it can create real changes in the joints, muscles, nerves, and overall mechanics of the neck and upper back.
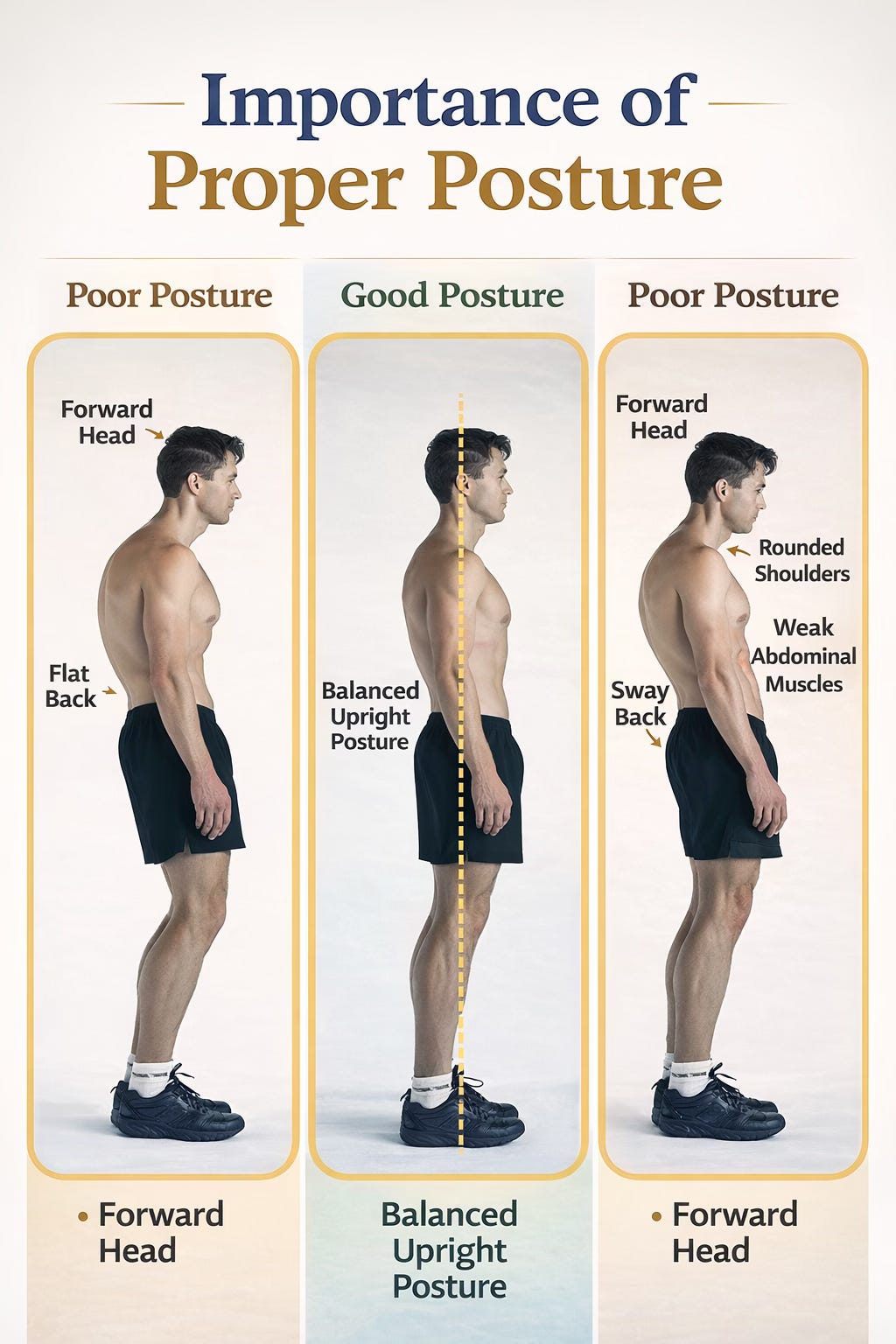
In a well-aligned posture, the head is stacked over the shoulders so that the weight of the skull is distributed efficiently through the spine. When the head moves forward, that balance changes. The body still needs to keep the eyes level so a person can look straight ahead, and to make that happen the neck begins to compensate in a very specific way. The upper part of the neck, especially around the base of the skull and the first two cervical vertebrae, begins to tip backward into extension, while the lower part of the neck tends to bend forward. In other words, forward head posture is not just “the whole neck leaning forward.” It is actually a combination of upper cervical overextension and lower cervical flexion, layered together in a pattern the body uses to keep the head upright and the gaze horizontal. Over time, this creates abnormal stress through several segments of the cervical spine and changes the natural curve of the neck (Hansraj, 2014; Mahmoud et al., 2019).
This matters because the neck is not just a flexible column; it is a finely tuned system of bones, discs, ligaments, muscles, and nerves that must work together with precision. The top of the neck is especially important because it contains joints that allow subtle nodding and rotational movements while also helping stabilize the head. When forward head posture becomes habitual, these upper segments are asked to do more than they were designed for. At the same time, the lower cervical spine is pushed into a position that can flatten or distort its normal lordotic curve. Clinical and biomechanical research shows that this pattern is associated with altered cervical alignment, increased joint loading, and reduced efficiency in how force is transferred through the neck (Mahmoud et al., 2019). That means the problem is not simply muscular tightness. The entire support system of the neck starts adapting around a faulty position.
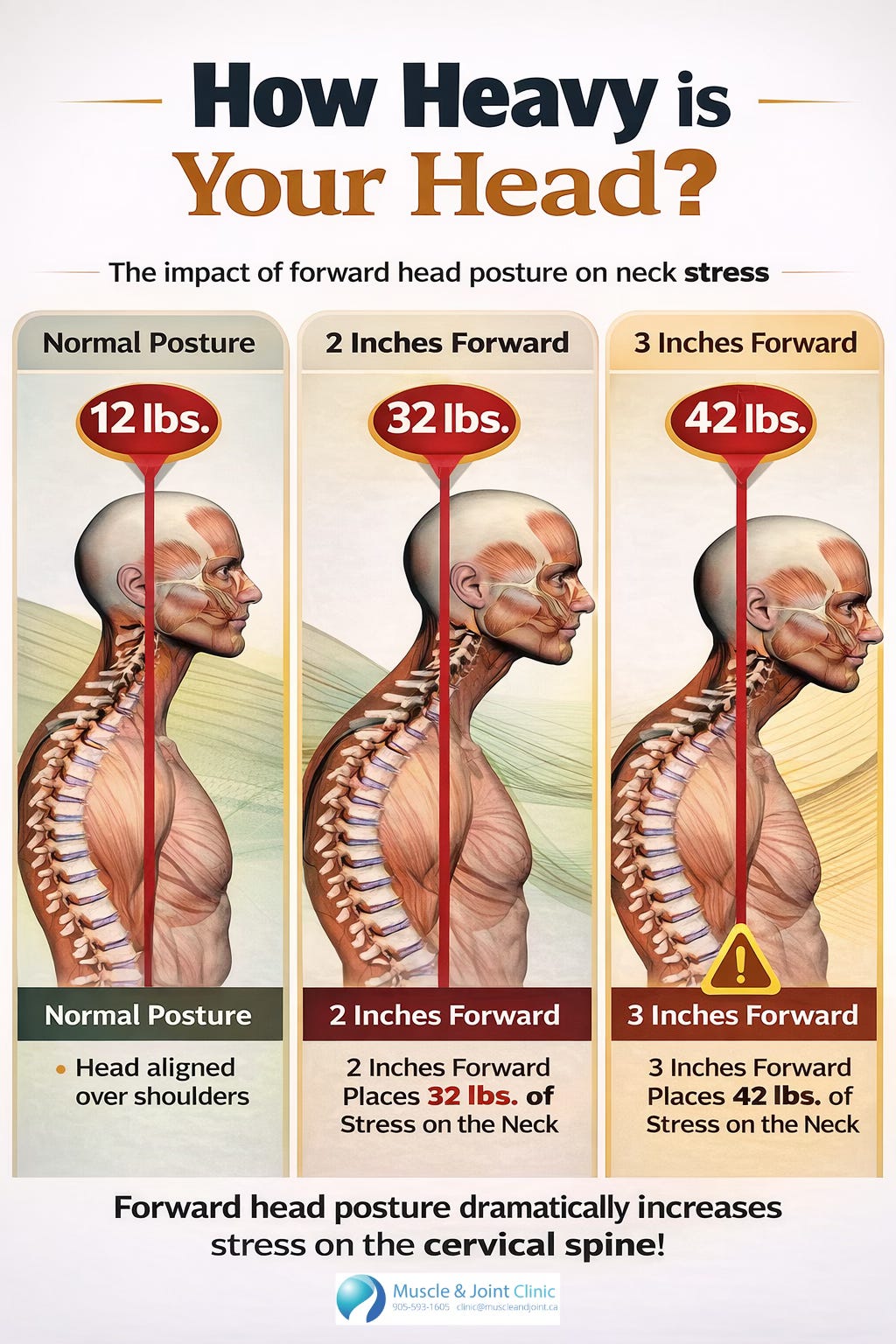
One of the easiest ways to understand this is to think about leverage. The human head weighs roughly 10 to 12 pounds when it is centered over the shoulders. But when it moves forward, even by a small amount, the muscles and joints of the neck have to work much harder to support it. This is because the farther the head moves from the body’s center of gravity, the larger the bending moment becomes. Hansraj (2014) popularized this concept by showing that as the head tilts or moves forward, the effective load seen by the cervical spine rises dramatically. Even if the exact number varies from person to person, the principle is clear: the farther forward the head goes, the greater the stress placed on the neck.
That stress is absorbed first by soft tissues. Some muscles become chronically short and overactive, while others become lengthened and weak. This is one of the most important physiological changes in forward head posture. The small muscles at the base of the skull, often called the suboccipital muscles, tend to shorten because the upper neck is being held in extension for long periods. These muscles are small, but they are rich in sensory receptors and play an important role in head position, balance, and fine motor control. When they stay shortened and tense, they can become a constant source of irritation and pain. At the same time, larger superficial muscles such as the upper trapezius, levator scapulae, sternocleidomastoid, and scalenes often become overworked as they try to support the head and neck in this altered position. In contrast, the deep neck flexors, muscles that are supposed to provide subtle support and stabilization from the front of the neck, often become less efficient and lose endurance. This creates the classic imbalance seen in many patients with neck pain: too much activity in the wrong muscles and not enough support from the ones that should be doing the job (Falla et al., 2007; Mahmoud et al., 2019).
These muscular changes help explain why forward head posture is so often linked with neck pain, stiffness, fatigue, and headaches. In adults, the relationship is no longer just theoretical. A systematic review and meta-analysis found that adults with neck pain demonstrate significantly greater forward head posture than asymptomatic adults, and that greater forward head posture is moderately associated with higher pain intensity and disability scores (Mahmoud et al., 2019). In practical terms, this means that the more the head drifts forward, the more likely it is that a person will report pain, limitations, or both. The relationship appears to be less consistent in adolescents, which may reflect the fact that structural and tissue adaptations take time to build. In adults and older adults, however, the connection is much stronger, likely because these patterns have had years to become ingrained (Mahmoud et al., 2019).
Another important consequence of forward head posture is reduced movement quality. People often assume that if they can still move their neck, their posture cannot be affecting function. But research suggests the opposite. Forward head posture has been associated with reduced cervical range of motion, particularly in rotation and extension, and with changes in how the upper and lower cervical spine contribute to movement (Quek et al., 2013; Mahmoud et al., 2019). This can make the neck feel stiff, but it can also make it less efficient. Rather than distributing movement smoothly across several joints, the body may start overusing some segments while underusing others. That uneven distribution can lead to localized irritation, sensitivity, and eventually pain.
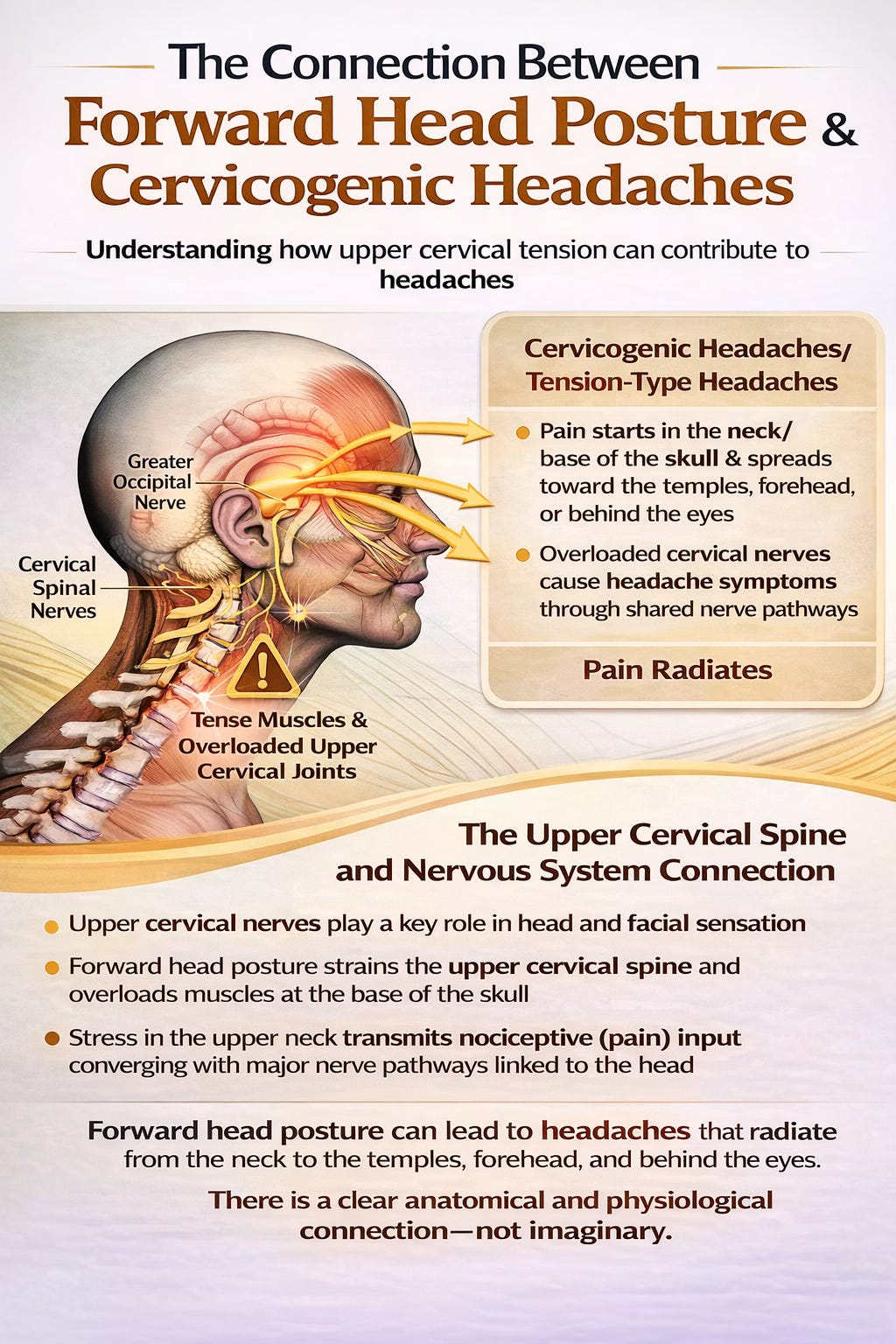
There is also a nervous system component. The upper cervical spine shares close relationships with nerves that contribute to head and facial sensation. When muscles at the base of the skull are constantly tense and upper cervical joints are overloaded, this can contribute to cervicogenic headaches and tension-type headache patterns. The pain does not arise because the brain itself is injured, but because nociceptive input from the upper neck converges with sensory pathways associated with the head. This is why people with forward head posture may report headaches that begin in the neck or base of the skull and spread toward the temples, forehead, or behind the eyes. The connection is anatomical and physiological, not imaginary. In many cases, the headache is one of the most important clues that the neck is under too much strain.
Forward head posture can also influence proprioception, which is the body’s ability to sense where it is in space. The neck contains an especially high density of proprioceptive input because head position is central to balance, eye control, and orientation. When the upper cervical muscles are constantly shortened and irritated, the sensory feedback they send to the brain can become less accurate. That may contribute to poor repositioning accuracy, altered balance, and a general sense that the neck feels “off” or hard to control. Even in people without severe pain, forward head posture has been linked to changes in postural control and static balance, suggesting that this postural pattern affects not only comfort but neuromuscular function as well (Lee, 2016).
The good news is that forward head posture is modifiable. But it usually does not respond well to a single stretch or a simple instruction to “sit up straight.” Because the problem involves joints, muscles, motor control, and daily habits, treatment tends to work best when it is multimodal. Research supports combining manual therapy with exercise rather than relying on one approach alone. Hands-on care can help restore mobility to restricted joints, reduce muscle guarding, and improve short-term comfort. Exercise then reinforces these gains by retraining the body to hold and control the head and neck more efficiently. Studies have shown that targeted neck exercise can improve sitting posture in people with chronic neck pain, while stabilization and postural correction programs can improve both pain and function (Falla et al., 2007; Mahmoud et al., 2019).
This makes sense physiologically. Manual therapy may help decrease local stiffness and reduce protective muscle tension, but if the person returns to the same poor mechanics without improved endurance and control, the old pattern often returns. Exercise addresses that missing piece by strengthening the deep stabilizers, improving scapular support, and teaching the body how to maintain a more efficient posture without overusing superficial muscles. This is especially important in people who spend long hours at a desk, on a laptop, or looking down at a phone, because their symptoms are not caused by one isolated event. They are the result of repeated loading in the same direction over months or years.
That is why long-term improvement often requires a broader strategy. Ergonomic changes matter. Screen height matters. The amount of time spent in sustained positions matters. Breaks matter. Sleep position can matter. Even breathing mechanics can matter, because people with upper chest-dominant breathing patterns often recruit the scalenes and sternocleidomastoid excessively, further feeding into neck tension. The more these daily factors are addressed, the more likely it is that treatment gains will hold.
Forward head posture is therefore not just a postural “bad habit.” It is a pattern of structural adaptation and functional compensation that can influence pain, movement, muscle performance, balance, and headache generation. It reflects the body’s attempt to manage repeated demands, but the price of that adaptation is often discomfort and dysfunction. Understanding it this way changes the conversation. Instead of blaming people for slouching, it helps explain why the body changes the way it does and why an effective solution needs to address both the physical tissues and the daily habits shaping them.
When patients understand that their head position affects much more than appearance, they are often more motivated to take the problem seriously. And they should. The neck is one of the most neurologically and mechanically important regions in the body. When it is under chronic stress, the effects can ripple outward into headaches, jaw tension, shoulder tightness, fatigue, and persistent pain. But with the right combination of hands-on care, corrective exercise, and consistent lifestyle changes, forward head posture can improve, and when it does, patients often notice benefits far beyond posture alone.
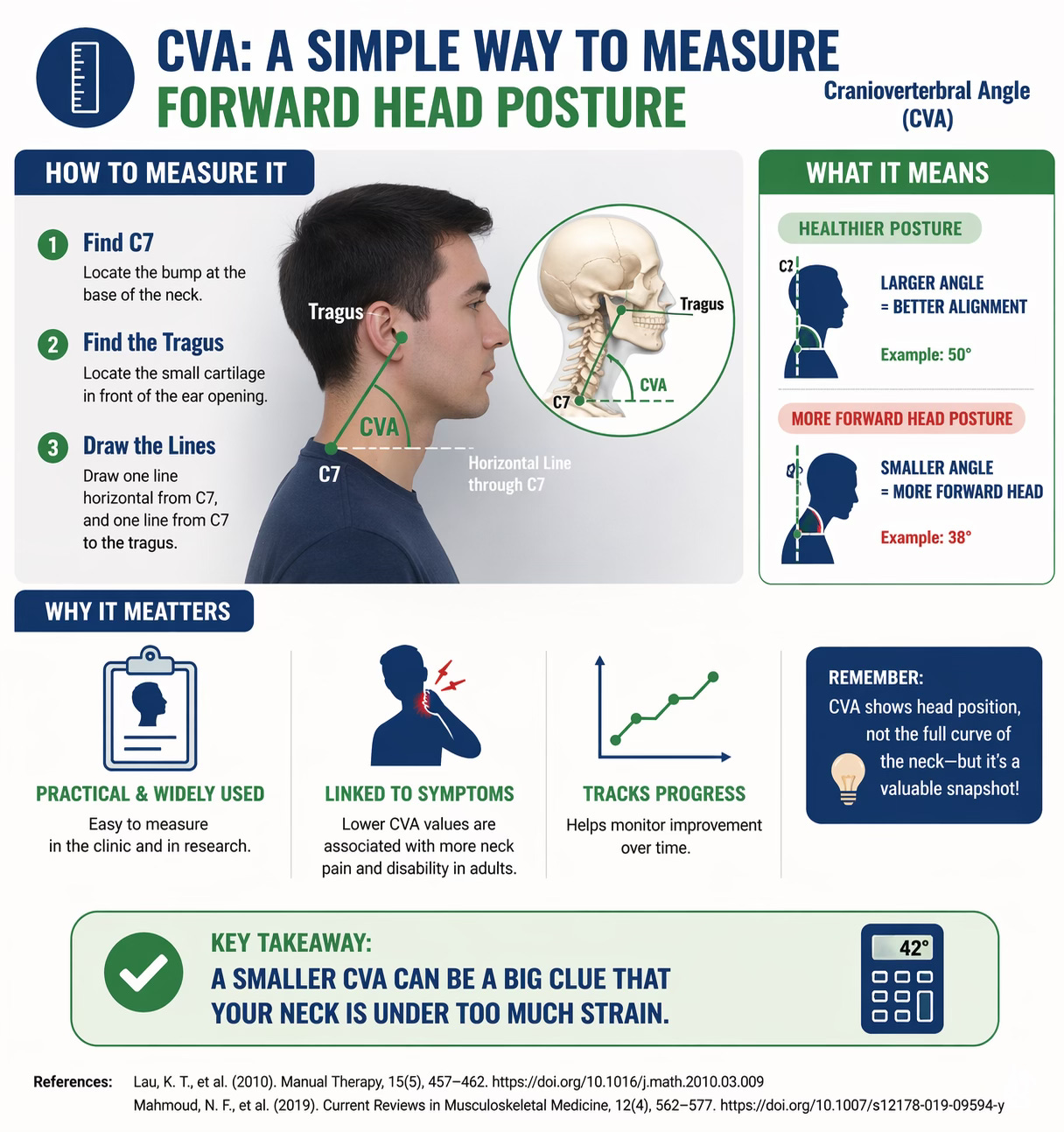
Clinically, one of the most common ways to measure forward head posture is by using the craniovertebral angle, or CVA. This angle is typically formed between a horizontal line through the seventh cervical vertebra and a line connecting that point to the tragus of the ear. A smaller angle generally indicates a more pronounced forward head posture. Although it does not provide a full picture of cervical curvature on its own, it is a practical and widely used measure in both research and clinical settings. Lower CVA values have repeatedly been associated with greater neck pain and disability in adults, making it a useful tool for tracking change over time (Lau et al., 2010; Mahmoud et al., 2019).
References
Falla, D., Jull, G., Russell, T., Vicenzino, B., & Hodges, P. (2007). Effect of neck exercise on sitting posture in patients with chronic neck pain. Physical Therapy, 87(4), 408–417. https://doi.org/10.2522/ptj.20060009
Hansraj, K. K. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International, 25, 277–279.
Lau, K. T., Cheung, K. Y., Chan, K. B., Chan, M. H., Lo, K. Y., & Chiu, T. T. W. (2010). Relationships between sagittal postures of thoracic and cervical spine, presence of neck pain, neck pain severity and disability. Manual Therapy, 15(5), 457–462. https://doi.org/10.1016/j.math.2010.03.009
Lee, J.-H. (2016). Effects of forward head posture on static and dynamic balance control. Journal of Physical Therapy Science, 28, 274–277. https://doi.org/10.1589/jpts.28.274
Mahmoud, N. F., Hassan, K. A., Abdelmajeed, S. F., Moustafa, I. M., & Silva, A. G. (2019). The relationship between forward head posture and neck pain: A systematic review and meta-analysis. Current Reviews in Musculoskeletal Medicine, 12(4), 562–577. https://doi.org/10.1007/s12178-019-09594-y
Quek, J., Pua, Y.-H., Clark, R. A., & Bryant, A. L. (2013). Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. Manual Therapy, 18(1), 65–71. https://doi.org/10.1016/j.math.2012.07.005