
Why Does My Arm Feel Numb, Weak, or Heavy?
Understanding Thoracic Outlet Syndrome (TOS)


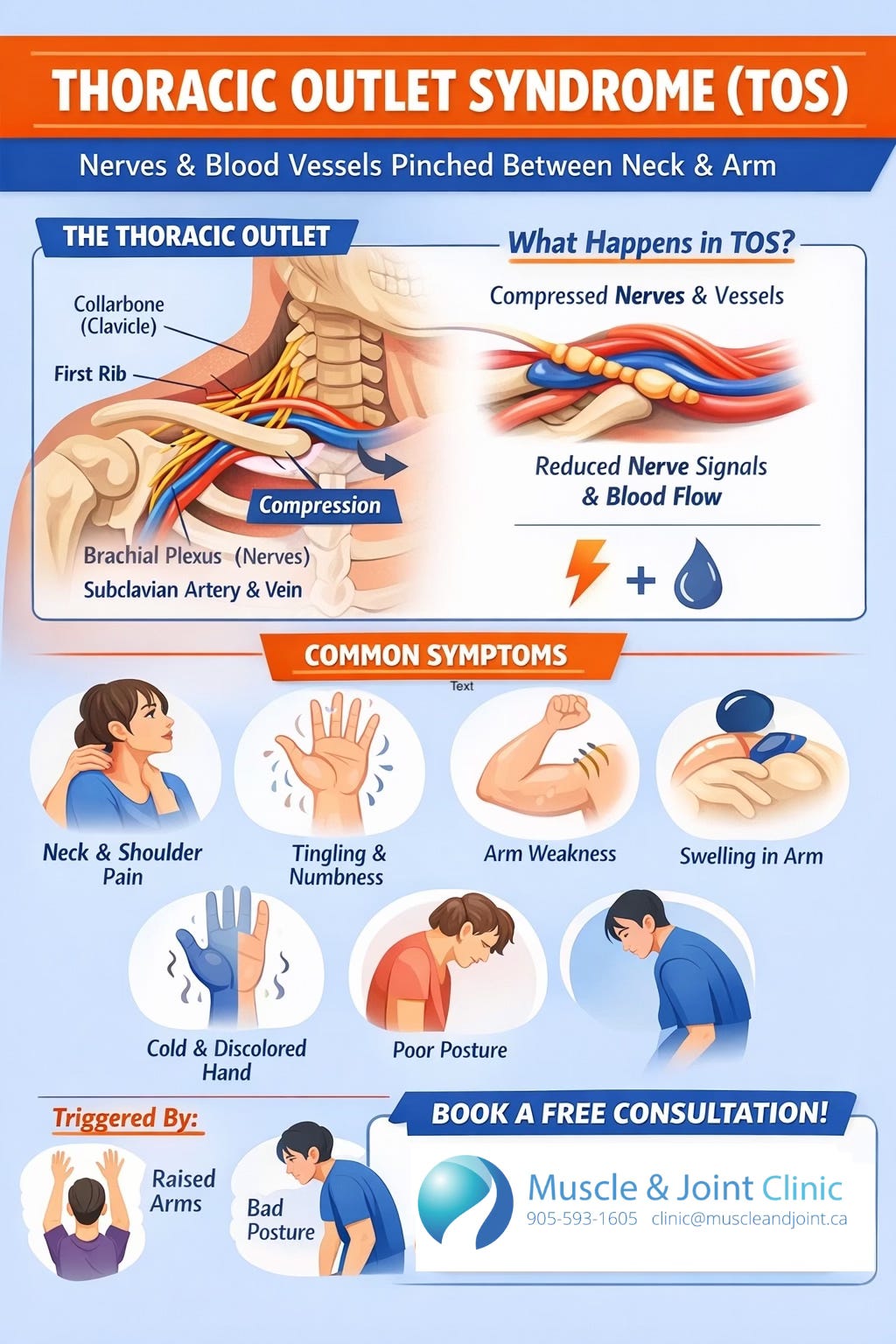
Thoracic Outlet Syndrome (TOS) is a condition in which important nerves and blood vessels become compressed, or “pinched,” as they travel from the neck into the arm through a narrow space between the collarbone and first rib. This space, known as the thoracic outlet, is surrounded by muscles, bones, and connective tissue, making it particularly vulnerable to narrowing or irritation. When compression occurs, it can interfere with normal nerve signaling and blood flow, leading to a range of symptoms. People with TOS commonly report neck and shoulder pain, tingling or numbness in the arm or hand, weakness, and in some cases changes in circulation such as swelling, discoloration, or a cold sensation in the affected limb (Li et al., 2021). These symptoms often worsen with certain positions or activities, particularly when the arms are raised overhead or when poor posture is maintained for extended periods.
TOS is generally divided into three main types depending on which structure is being compressed.
The most common form, accounting for approximately 95% of cases, is neurogenic TOS, which involves pressure on the brachial plexus, a network of nerves that controls movement and sensation in the arm. This type typically presents with pain, tingling, numbness, and weakness in the arm and hand (Li et al., 2021).
Venous TOS, which makes up about 4% of cases, occurs when the subclavian vein is compressed and may lead to symptoms such as arm swelling, a feeling of heaviness, and a bluish discoloration of the skin.
The rarest but most serious form is arterial TOS, affecting roughly 1% of individuals, where compression of the subclavian artery can reduce blood flow, causing the arm or hand to feel cold, pale, fatigued, or weak (Li et al., 2021).
Although these categories are useful, it is important to note that symptoms can overlap, especially when multiple structures are affected at the same time.
The causes of TOS are often multifactorial, meaning that several contributing factors are usually involved. Research suggests that approximately 70% of cases are related to soft tissue issues such as tight or overactive muscles, scar tissue, or postural dysfunction, while the remaining 30% are associated with structural or bony differences, such as an extra rib (cervical rib) or abnormalities of the clavicle (Li et al., 2021).
Poor posture is one of the most common contributing factors in modern lifestyles. A forward head position and rounded shoulders can reduce the available space in the thoracic outlet by shortening key muscles like the scalenes and pectoralis minor, increasing the likelihood of compression.
Repetitive overhead activities, such as those seen in athletes or certain occupations, can further aggravate the condition by causing muscle tightness, inflammation, or hypertrophy.
Trauma is another important factor, particularly injuries such as whiplash from motor vehicle accidents or fractures of the collarbone, which can alter the structure of the thoracic outlet and contribute to nerve or vessel irritation (Li et al., 2021; Citisli, 2015).
Compression in TOS most commonly occurs in three specific anatomical areas. The first is the scalene triangle, located between muscles in the side of the neck and the first rib, where the nerves and artery pass through. The second is the costoclavicular space, which lies between the collarbone and the first rib and contains both nerves and blood vessels. The third is the subcoracoid or pectoralis minor space, located beneath a chest muscle where structures pass into the arm. Each of these areas can become narrowed due to posture, muscle tightness, or structural variations, contributing to the development of symptoms (Li et al., 2021). Understanding these regions helps guide both diagnosis and treatment strategies.
Diagnosing TOS can be complex because there is no single definitive test. Instead, healthcare providers rely on a combination of patient history, physical examination, and sometimes imaging. During the assessment, clinicians evaluate posture, movement patterns, and areas of tenderness, and they may use specific arm and neck positions to reproduce symptoms. Common clinical tests, such as the Elevated Arm Stress Test (EAST), Upper Limb Tension Test (ULTT), and Adson’s test, can help support the diagnosis, although they are not perfectly accurate on their own (Li et al., 2021). Imaging studies such as X-rays, CT scans, or MRI may be used to identify structural abnormalities or rule out other conditions like cervical disc issues or nerve entrapments elsewhere in the arm. In cases where vascular involvement is suspected, ultrasound or angiographic studies may be used to assess blood flow and detect any compression of the arteries or veins (Li et al., 2021).
For most individuals, the first line of treatment is conservative, meaning non-surgical. Evidence shows that a combination of physical therapy, activity modification, and education can lead to improvement in a large percentage of patients, with reported success rates ranging from approximately 59% to 88% (Li et al., 2021). Physical therapy focuses on correcting posture, improving shoulder and neck mechanics, and restoring balance between tight and weak muscles. Stretching exercises target shortened muscles such as the scalenes and pectoralis minor, while strengthening exercises focus on stabilizing the shoulder blades and improving overall alignment. Hands-on therapies, ergonomic adjustments, and education on daily habits, such as workstation setup, sleep positioning, and movement patterns, are also essential components of care (Citisli, 2015). These strategies aim to reduce pressure on the affected structures and prevent recurrence of symptoms.
When conservative care does not provide sufficient relief, additional treatments may be considered. Injection therapies, including local anesthetics, corticosteroids, or botulinum toxin, may be used to reduce muscle tension and inflammation around the compressed structures. While some patients experience short-term improvement with these interventions, results can vary depending on the underlying cause and duration of symptoms (Li et al., 2021). In more severe or persistent cases, particularly when there is significant nerve damage or compromised blood flow, surgical intervention may be recommended. Procedures such as first rib resection or removal of tight muscles (scalenectomy) aim to create more space in the thoracic outlet and relieve pressure. Surgical outcomes are generally favorable in carefully selected patients, with success rates reported to be as high as 90% in some studies (Li et al., 2021).
Thoracic Outlet Syndrome is a complex condition that results from compression of nerves or blood vessels between the neck and shoulder. It often develops due to a combination of posture, muscle imbalance, repetitive strain, or structural factors. Although it can cause significant discomfort and functional limitations, early recognition and appropriate management are key to recovery. Most individuals respond well to conservative treatment, especially when it focuses on improving posture, movement, and muscle balance. A comprehensive and individualized approach, often involving multiple healthcare professionals, offers the best chance for long-term relief and improved quality of life.
References (APA Style)
Citisli, V. (2015). Assessment of diagnosis and treatment of thoracic outlet syndrome, an important reason of pain in upper extremity, based on literature. Journal of Pain Relief, 4(2), 173. https://doi.org/10.4172/2167-0846.1000173
Li, N., Dierks, G., Vervaeke, H. E., Jumonville, A., Kaye, A. D., Myrcik, D., Paladini, A., Varrassi, G., Viswanath, O., & Urits, I. (2021). Thoracic outlet syndrome: A narrative review. Journal of Clinical Medicine, 10(5), 962. https://doi.org/10.3390/jcm10050962