
Why That Inner Knee Pain Won’t Go Away: The Pes Anserine Explained


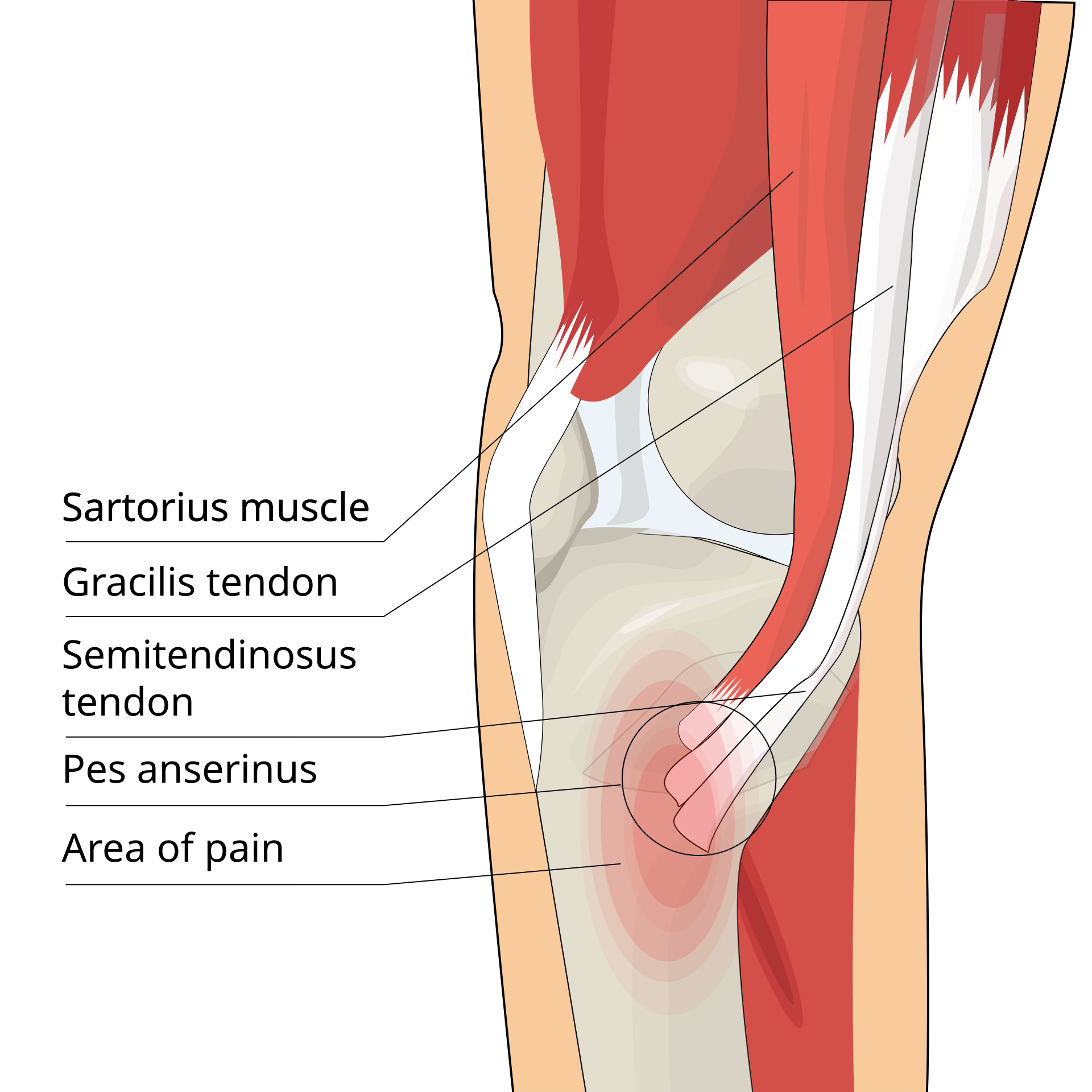
The pes anserine complex is an important but often overlooked area on the inside of the knee. The term “pes anserine” means “goose foot,” which describes the way three tendons spread out and attach to the upper inner part of the shinbone, just below the knee joint. These tendons come from three muscles: the sartorius, gracilis, and semitendinosus. Although each of these muscles has its own role, together they help support the inner knee, assist with bending the knee, and contribute to control during walking, climbing, pivoting, and changing direction. Beneath these tendons sits a small fluid-filled sac called the pes anserine bursa, which helps reduce friction as the tendons glide over the bone. When this area becomes irritated, either the tendons, the bursa, or both can become painful.
This region matters because it acts like a stabilizing support system for the inside of the knee. Every time a person bends the knee, twists, slows down, or pushes off the ground, the pes anserine complex helps guide and control that movement. It is especially active during motions that combine knee bending with rotation, which is why it is commonly irritated in active people and athletes. It is also an area that can become overloaded in everyday life, especially in people who spend long periods sitting, have weak hip muscles, tight hamstrings, altered walking mechanics, or extra body weight that increases strain through the knee.
When the pes anserine complex becomes irritated, the symptoms are usually quite specific. People often describe pain on the inner side of the knee, usually a little below the actual joint line rather than directly in the center of the knee. The discomfort may feel like a nagging ache, a tender soreness, or sometimes a burning or pulling sensation. Many people notice it most when getting up after sitting for a while, kneeling down, squatting, or trying to bend the knee forcefully. Some feel pain during prayer positions, lunges, or when turning quickly on a planted foot. Others notice that the inside of the knee feels sore to touch, especially when pressing the upper inner shin. In some cases, the pain can spread slightly toward the back of the knee, especially if the semitendinosus portion of the complex is involved. A person may still be able to walk and function, but the discomfort tends to linger and become annoying because it does not completely settle.
One reason this condition is often confusing is that it can mimic other knee problems. Inner knee pain makes many people worry about a meniscus tear, arthritis, or ligament injury. However, pes anserine irritation often behaves differently. For example, a person may have pain when kneeling, twisting, or standing up from a chair, but no true locking, no major swelling, and no sense that the knee is giving way. Stairs may or may not hurt, depending on the severity and the movement pattern, and the pain is often more tender and localized below the inner joint line than within the joint itself. This is one reason why a proper assessment matters: not all inner knee pain is coming from the same structure.

There are many reasons the pes anserine complex can become irritated, but most cases come down to overload rather than a single dramatic injury. Repetitive pivoting is a common culprit. Sports such as pickleball, tennis, soccer, basketball, badminton, and volleyball all involve quick changes of direction, cutting, and rotation through the knee. Running, especially hill running or sudden increases in mileage, can also stress this area. In the gym, it may flare up with deep squats, lunges, step-ups, leg presses, or poorly controlled lower body training. Even non-athletes can develop this problem from repetitive stair climbing, prolonged kneeling, deconditioning, or movement compensations caused by tight muscles or weak hips.
Certain risk factors make pes anserine irritation more likely. Tight hamstrings can increase tension through the semitendinosus tendon. Weak gluteal muscles can reduce control of the thigh and pelvis, causing the knee to collapse inward or rotate more than it should during activity. Limited hip mobility can shift rotational stress down into the knee. Flat feet or altered foot mechanics can change how the leg loads with each step. Carrying extra body weight can increase force through the inside of the knee, especially during sports or repetitive bending. It is also more common in people who suddenly return to activity after a period of relative inactivity, because the tissues are not yet conditioned for the load being placed on them.
In sports medicine, this type of condition is usually considered an overuse injury. That means it develops gradually, often over weeks or months, as the tendons and surrounding tissues are exposed to more stress than they can recover from. A pickleball player, for example, may start feeling a slight inner knee ache after games, then notice that the pain lingers longer and becomes more noticeable when standing after sitting. A runner may feel it after speed work or hill sessions. A gym-goer might first notice it during lunges or when lowering into a squat. A soccer player could feel it after repeated planting and cutting on the same leg. The common thread is repeated stress without enough recovery or without enough strength and mobility support from the rest of the body.
The anatomy also helps explain why this region is so sensitive. The sartorius helps with hip flexion, abduction, and external rotation while also assisting knee flexion. The gracilis helps bring the leg inward and assists with knee bending. The semitendinosus, part of the hamstrings, helps bend the knee and extend the hip. These muscles all pull in slightly different ways, but they meet at a shared insertion point along the inner upper tibia. That means the area is constantly dealing with combined forces from the hip and knee. If one or more of these muscles becomes tight, weak, fatigued, or overworked, the shared insertion site becomes vulnerable to irritation. If the bursa underneath becomes inflamed, the area can become even more tender and painful with pressure or repetitive motion.
Treatment for pes anserine problems is usually very successful, but it works best when the real causes are addressed instead of simply masking the pain. Relative rest is often helpful early on, but complete inactivity is usually not necessary and often not ideal. Activity modification is more useful. That may mean temporarily reducing pivoting sports, shortening workouts, or avoiding deep knee bending until symptoms calm down. Soft tissue treatment can help reduce tension in the hamstrings, adductors, and surrounding muscles. Stretching may be useful if there is clear tightness, especially in the hamstrings or hip flexors, but it needs to be done thoughtfully so the irritated tissue is not constantly aggravated. Strengthening the glutes, hips, and core is often one of the most important parts of recovery, because better control from the pelvis and hip reduces the stress being dumped into the inside of the knee. Taping or a brace can sometimes help with short-term support during sport or work, but these are usually adjuncts rather than the full solution.
Recovery time depends on how long the symptoms have been present, how irritated the tissues are, and whether the underlying mechanics are corrected. Mild cases may improve within a few weeks, while more persistent cases can take longer. The encouraging part is that most people do well when treatment is targeted properly. Once the irritation settles and strength and mobility improve, people can usually return to activity without major limitations. The key is not simply waiting for the pain to disappear, but building the body’s capacity so the same overload pattern does not keep coming back.
The pes anserine complex may be small compared with larger knee structures, but it plays a major role in how the knee handles load, rotation, and control. When it becomes irritated, it often serves as a clue that something in the overall movement system is not working as efficiently as it should. For some people, it is a sports injury. For others, it is a lifestyle and mechanics problem. In either case, understanding the anatomy and the pattern behind the pain is the first step toward getting better.